Download
1 / 28
370 likes | 879 Views
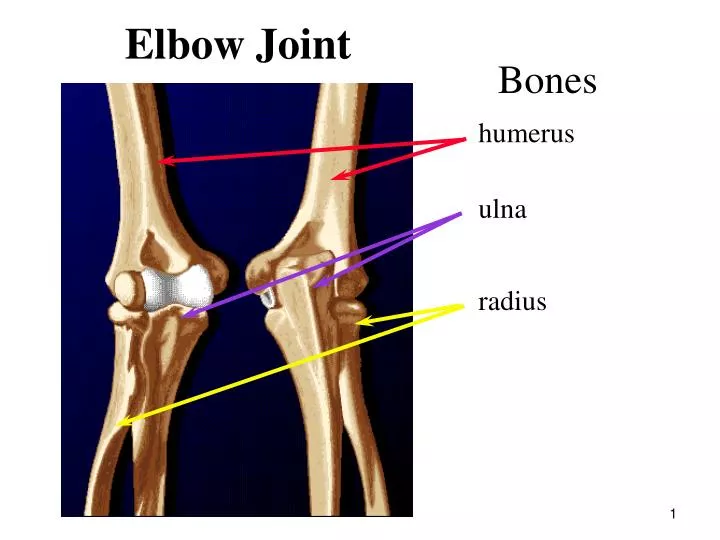
Elbow Joint. Bones. humerus. ulna. radius. Elbow Joint. A very stable joint that assists shoulder in application of force and controlling placement of hand in space. humeroulnar joint. humeroradial joint. Asymmetrical structure of trochlea creates angulation of ulna

E N D
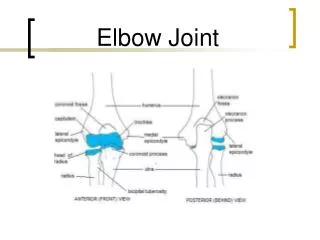
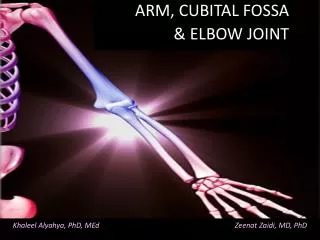
Elbow Joint Bones humerus ulna radius
Elbow Joint A very stable joint that assists shoulder in application of force and controlling placement of hand in space humeroulnar joint humeroradial joint Asymmetrical structure of trochlea creates angulation of ulna when extended known as the carrying angle proximal radioulnar joint
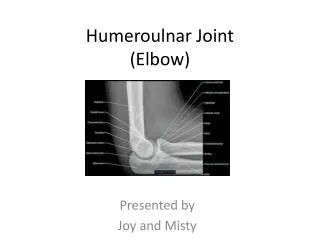
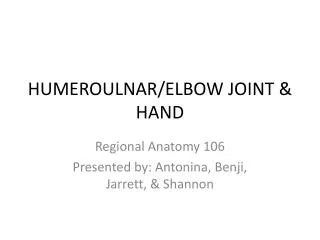
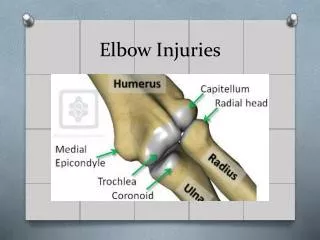
Elbow Structures coronoid fossa radial fossa lateral epicondyle trochlea capitulum medial epicondyle coronoid process Anterior View
Anterior view of right elbow joint Elbow Ligaments Varus Valgus annular ligament holds radius up into the elbow jt. medial/ulnar collateral resists valgus stresses ulnar collateral is taut in all joint positions valgus support very important since most forces are directed medially (creating a valgus force) lateral/radial collateral resists varus stresses because varus stresses are rare support from these ligaments is less significant
Elbow ROM flexion/extension 145º active, 160º passive need 100-140º to perform ADL’s (e.g., reach back of head to comb hair need 140º only 15º needed to tie a shoe) supination/pronation 85º supination; 70º pronation need 50º supination & 50º pronation to perform ADL’s
Elbow Flexors biceps brachii multi-articular muscle whose effectiveness is dependent on position of shoulder & radioulnar jts Flexors are almost twice as strong as the extensors making us better pullers than pushers brachialis brachioradialis (Used more in rapid mvmts or against resistance) Note: brachialis is the MOST EFFECTIVE elbow flexor! biceps brachii not effective when pronated
Elbow Extensors triceps brachii long head is bi-articular so its force production dependent on shoulder position lateral head is strongest yet is relatively inactive unless acting against resistance anconeus medial head is the ‘workhorse’ of this group active in all positions
Radioulnar Joints biceps brachii supinator active in rapid mvmts or against large loads always active Supination Pronation pronator teres active in rapid mvmts or against large loads pronator quadratus always active
Forearm muscle contribution in throwing Biceps brachii & brachialis active to flex elbow (& abduct shoulder) Biceps most susceptible to strain during this phase triceps activity drops off sharply - biceps brachii and brachialis quickly become active to decelerate elbow triceps brachii becomes active to extend elbow (some dispute this)
Injury potential in forearm Mainly a consequence of repetitive activities dislocations are possible often accompanied by fracture of medial epicondyle myositis ossificans of brachioradialis deposits of ectopic bone in muscle 2nd most common site behind quads high velocity overhead movements (e.g., throwing, tennis serve) large tensile forces developed medially large compressive forces developed laterally large shear forces developed posteriorly this is created by the development of a large VALGUS force on elbow during late cocking and early acceleration
Medial Epicondylitis linked to movements containing high velocity valgus extension mechanism large valgus torque near maximal external rotation resisted by a large varus torque generated by the soft tissue in the elbow
Little Leaguer’s Elbow • medial epicondylitis • medial strain imparted during the initial forward phase of throw as hand and elbow lag behind trunk and shoulder • curveball pitching will magnify this medial strain throughout pitch and therefore is not recommended for young pitchers
Medial Elbow Injuries (“Little Leaguer’s Elbow”) Sprain or rupture of ulnar collateral ligaments medial epicondylitis tendinitis of wrist flexors avulsion fractures of medial epicondyle osteochondritis dissecans to the capitulum (a lesion in the bone and articular cartilage) where the radial head is pushed up into the capitulum due to the compressive load developed from the valgus force
Tennis elbow • lateral epicondylitis -inflammation/microdamage to tissues on the lateral side of the humerus, 30%-40% of tennis players will develop some amount of this injury • causes include poor technique and equipment • e.g. off-center shots and rackets strung too tightly • The pain is exacerbated by activities involving extension of the wrist. These include lifting a suitcase, shaking hands, turning doorknobs, etc
The Wrist and Hand Radiocarpal Joint Distal Radioulnar Joint I Carpals WRIST - radiocarpal joint condyloid joint ulna makes no contact with carpals but floats on disc so it does not influence wrist mvmt during supination/pronation II Metacarpals P M III Phalanges D IV V
The scaphoid may be one of the most important carpals because it supports the weight of the arm and transmits the forces between the hand and the forearm Radiocarpal jt is the articulation between the scaphoid & radius scaphoid Midcarpal joint Wrist ROM flexion: 70-90º need 10-15º for ADL’s extension: 70-80º need 35º for ADL’s ROM reduced when fingers are flexed
Radial & Ulnar Deviation proximal row of carpals glides over distal row ROM radial dev. 15-20º ulnar dev. 30-40º
CMC of thumb is a saddle jt that allows flex/ext, ab-/adduction & rotation these movements permit thumb to touch each finger (known as opposition) opposition is very important in all gripping & prehension tasks Carpometacarpal (CMC) jt Concave transverse arch metacarpals to facilitate gripping
Metacarpophalangeal (MCP) jts MCP of thumb is a hinge jt allowing only flex/ext MCP of fingers is a condyloid jt permitting flex/ext and ab-/adduction
extensor carpi radialis longus extensor digitorum extensor carpi radialis brevis extensor carpi ulnaris Wrist Extensors NOTE: Origin on lateral epicondyle Because the extensors act on the elbow jt, elbow jt pos. will influence extensor output
flexor carpi radialis flexor carpi ulnaris Wrist Flexors all fusiform muscles NOTE: Origin on medial epicondyle palmaris longus strongest flexor strength increased by encasing the pisiform in its tendon such that it becomes a sesamoid bone that improves the mechanical advantage of the muscle Absent in 13% of population
Radial Deviation - created by the radial muscles Extensor carpi radialis longus & brevis Flexor carpi radialis Ulnar Deviation - created by the ulnar muscles Extensor carpi ulnaris Flexor carpi ulnaris
Most of the muscles acting on wrist & fingers originate outside of the hand in the region of the elbow so they are known as extrinsic muscles Tendons are held in place on the dorsal and palmar sides by the extensor & flexor retinaculumrespectively (a thick band of fibrous tissue running transversely across the wrist) intrinsic muscles of the hand include 4 muscles on thumb forming the thenar eminence and 3 muscles on the pinky forming the hypothenar eminence
Grip strength related to wrist position strongest when wrist is slightly ulnar deviated and hyperextended grip @ 40º extension is 3X stronger than in 40º flexion neutral grip is safest position that minimizes strain on wrist structures power grip utilizes extrinsic muscles precision grip utilizes intrinsic muscles Thumb position greatly influences grip thumb in plane of the hand in an adducted position such that fingers flex around object a power grip is created thumb is positioned perpendicular to hand and moved into opposition a precision grip is created
Wrist actions in activities dynamic actions golf/baseball swing: active radial and ulnar deviation in the preparatory and power phases respectively static actions piano playing/typing: must maintain a stable, static position in order to maximize finger action
Wrist/Hand Injuries falls - broken with outstretched hand forces wrist into position of extreme extension or flexion sprain wrist ligaments strain wrist flexors fracture schaphoid fracture distal radius one of the most frequently fractured areas of the body because of its lower density and the size of the forces it usually accommodates Overuse injuries - repetitive strain injuries tenosynovitis of radial flexors and thumb muscles from canoeing, rowing, tennis, and fencing medial epicondylitis due to overuse of wrist flexors
Carpal Tunnel Syndrome repeated wrist flexion/extension may inflame wrist flexor tendons to the point that they apply pressure and constrict the median nerve which innervates the radial side of the hand (thenar muscles) wrist stabilization in a neutral position is recommended as treatment or prevention often using an external device Ulnar Nerve Injuries occurs due to trauma to the elbow note that this nerve is not encased in the carpal tunnel Carpal Tunnel tunnel formed by the carpals (floor and walls) and the roof is formed by a transverse ligament and retinaculum
Basic Steps in Open Carpal Tunnel Release Step 1 A small incision, usually less than 2 inches, is made in the palm of the hand. In some severe cases, the incision needs to be extended into the forearm another 1/2 inch or so. Step 2 After the incision is made through the skin, a structure called the palmar fascia is visible. An incision is made through this material as well, so that the constricting element, the transverse carpal ligament, can be seen. Step 3 Once the transverse carpal ligament is visible, it is cut with either a scalpel or scissors, while making sure that the median nerve is out of the way and protected. Step 4 Once the transverse carpal ligament is cut, the pressure is relieved on the median nerve. Step 5 Finally, the skin incision is sutured. At the end of the procedure, only the skin incision is repaired. The transverse carpal ligament remains open and the gap is slowly filled by scar tissue.