Download
1 / 49
490 likes | 748 Views
Washington Update NASMHPD & NASDDDS Legal Divisions’ Meeting Alexandria, Va. November 13, 2012. Joel E. Miller Senior Director of Policy and Healthcare Reform National Association of State Mental Health Program Directors. Outline of Presentation.

E N D
Washington UpdateNASMHPD & NASDDDSLegal Divisions’ Meeting Alexandria, Va.November 13, 2012 Joel E. Miller Senior Director of Policy and Healthcare Reform National Association of State Mental Health Program Directors NASMHPD, 2012
Outline of Presentation • The Election and Impact on Congress and Key Senate and House Committees • Impact of the Election on Implementation of the Affordable Care Act (ACA) - Health Insurance Exchanges - Essential Health Benefits - State Medicaid Expansion Activities • The “Fiscal Cliff” and Discussion on SAMHSA’s Budget • Impact of the Election on Overall Health Care Policy and Behavioral Health Care Policy NASMHPD, 2012
Mandate or No Mandate? • While the election left Washington’s political power balance the same, there are some notable changes in the political landscape. • President Obama won re-election by a comfortable margin in the electoral college – 332 to 206 and the popular vote by 3.1 million. • U.S. Senate – Democrats increased majority by 2 – make up is 55 Democrats/Independents and GOP at 45 members. • U.S House – remains essentially the same with the Republicans holding their strong majority over the Democrats at 238 to 195. The final tallies -- 84 new House members - 49 Dems and 35 Republicans. NASMHPD, 2012
The New Senate Emerges as Many Senators are Leaving Office • Daniel Akaka (D-HI) – retiring Olympia Snowe (R-ME) – retiring • Jeff Bingaman (D-NM) – retiring Jim Webb (D-VA) -- retiring • Scott Brown (R-MA) – lost re-election • Kent Conrad (D-ND) – retiring • Kay Bailey Hutchinson (R-TX) retiring • Herb Kohl (D-WI) retiring • Jon Kyl (R-AZ) retiring • Joe Lieberman (I-CT) retiring • Richard Lugar (R-IN) lost in primary election • Ben Nelson (D-NE) retiring NASMHPD, 2012
Political Dynamics House of Representatives • Even with House Republicans maintaining their majority, retirements and party term limits could lead to as many as a dozen full committee chairmanship and ranking member changes in the 113th Congress. • And that doesn't include Republican and Democratic vacancies at the top of almost 30 subcommittees. Negotiating new party ratios on committees shouldn't be a big problem for the GOP, given the slight Democratic gain in overall seats. • Here's a look at the likely work plan for the 2 House committees with the most jurisdiction over health matters: Committee Republicans approved countless measures in the current Congress signaling their displeasure with the Obama Administration’s health care overhaul. They’re expected to pick up where they left off in the next Congress. • When "World News" anchor Diane Sawyer asked if there would be any more votes to repeal the law, Speaker Boehner said "the election changes that" and "Obama-care is the law of the land.“ In a way, Boehner was just acknowledging the obvious: With President Barack Obama back in the White House for another four years, and the Senate still firmly in Democratic hands, a full repeal of the health care law is out of the question.
Gubernatorial Races and Make Up of State Legislatures • Democrats took control of state legislatures in Maine, Minnesota, Colorado, New York and Oregon, according to the NCSL. The GOP took control of legislatures in Arkansas, Wisconsin and Alaska. • In New Hampshire, Democrat Maggie Hassan’s victory means the state will likely expand Medicaid as called for by the law and create an insurance exchange. • The prospects for smooth implementation of the law in Indiana decreased with the election ofMike Pence (R) who has said he opposes starting a state-based exchange. He favors expanding Medicaid only if the state can limit benefits and ask recipients to pay higher premiums. • In North Carolina, the election of Republican Pat McCrory means that state is unlikely to expand Medicaid. • Democrat Gov. Steve Bullock in Montana’s is undecided on the Medicaid expansion and the creation of an insurance exchange. Republican Gov. Gary Herbert of Utah, who was re-elected, opposes expanding Medicaid. Republican Gov. Jack Dalrymple of North Dakota, who was also re-elected, has not taken a position on Medicaid expansion and has opposed a state exchange. • Some Democratic incumbents who won re-election favor expansion, including Jack Markell in Delaware and Peter Shumlin in Vermont. NASMHPD, 2012
The ACA Could Be Attacked on 3 Fronts: Political, Policy and Legal • Slow it down in the states. Challenge it in the courts. Try to get Congress to repeal its most vulnerable elements, and attempt to chop its funding at every opportunity. • Republicans and other opponents aren’t just going to wave the white flag. They will still try to repeal parts of the law, ramp up investigations and target sections they see as legally vulnerable. • Of the health-related proposals for which CBO has published an estimate, the one with the largest savings would repeal provisions of the ACA that expand health insurance coverage (while leaving other provisions of that law unchanged). That option would decrease spending by nearly 15 percent in 2020 and would reduce the deficit by roughly $150 billion in that year, according to estimates by CBO and the staff of the Joint Committee on Taxation (JCT). • The option would also increase the number of people without health insurance coverage by an estimated 29 million in 2020. NASMHPD, 2012
ACA and GOP Political Opposition Strategy“Getting Under the Hood” • We will see a targeted or “rifle shot” approach at particular aspects of the ACA that are unpopular. Indeed, any budget negotiations risk raiding the funding of the ACA. • One fight already under way centers on whether people will be able to get subsidies in health exchanges that are run by the feds, or only when the states themselves run them. • Republican aides have said that GOP members were eyeing exchange subsidies, particularly for those with higher incomes. • Once you start rolling back the subsidies, you really are starting to affect affordability for the population to make the marketplace work. Some of the law’s popular provisions –namely, requiring insurers to cover people with pre-existing conditions – will raise costs by bringing sick people into the system. ACA tries to offset that effect with the individual mandate, which should bring more healthy people into the system. • Some governors are saying they may just not move ahead to set up the health exchanges. But even then, all that happens is that the Feds would set up the exchanges for them. NASMHPD, 2012
ACA and GOP Opposition Strategy • Among the most likely first targets post-election by Congressional GOP: the 2.3 percent medical device tax that kicks in at the beginning of next year and the loathed Independent Payment Advisory Board (IPAB). • Senate Republican aides have said they would try to at least delay the medical device tax in any year-end deal on the fiscal cliff. The tax was intended to be the industry’s contribution to the health care law’s insurance expansions that are expected to deliver new business. Some Democrats, including the delegations of med-tech heavy Minnesota and Massachusetts, have said they support repealing the tax, although a repeal bill that passed the House would pay for it by raiding exchange subsidies. • Majority Leader Eric Cantor sent a letter to Republican colleagues pledging a bill in the new Congress to repeal the IPAB, the 15-member board intended to propose ways to control Medicare spending if it exceeds a certain rate and Congress fails to act. • Funding for the Center for Medicare and Medicaid Innovation, which is testing a variety of payment reform pilots, is a likely target, in addition to the Prevention and Public Health Fund, which some House Republicans have called a “slush fund”. NASMHPD, 2012
Here are Some Potential Land Mines to Watch for Over the Next Two Years: • Legal Battles. There’s also a pending legal challenge from Liberty University against the requirement that would make most businesses with more than 50 workers provide health coverage or pay a fine. Liberty says that requirement is unconstitutional – and yes, it has vowed to fight all the way to the Supreme Court. • State Opposition.Indeed, securing cooperation from the states on health care reform generally promises to be a major headache for the Obama Administration going forward. Republicans appear to have picked up at least one governorship and to have made gains in some state houses. Alabama, Montana, and Wyoming passed anti-Obama-care amendments, although Florida defeated a similar ballot measure. These measures are purely symbolic. • The Administration will have to confront this resistance firmly, but also work with pragmatic-minded officials to make the ACA work for all Americans. NASMHPD, 2012
Threats To The ACA • State Opposition. High on the Administration’s agenda must be helping the states to understand why they should embrace the ACA Medicaid expansion, which was made optional through the Supreme Court’s NFIB decision. The states have every reason to expand Medicaid. The federal government initially funds 100 percent of the expansion, and the state’s share will never exceed 10 percent. • Hospitals in rejectionist states will face an unmanageable uncompensated care burden just as their Medicare funding is cut, and managed care companies will lose out on a lucrative Medicaid managed care market in states that reject expansion. • Challenges to the Preventive Services Contraceptive Mandate. Over two dozen lawsuits are pending challenging the preventive services contraception mandate. Several of these have been dismissed pending the Administration working out a compromise with religious institutions that object to covering contraception. Such a compromise has been promised, and this promise should be honored. On the other hand, the Administration is facing a number of lawsuits brought by for-profit businesses claiming exemption from the mandate because of the religious beliefs of their owners. In two of these lawsuits a preliminary injunction has been issued. NASMHPD, 2012
Threats To The ACA • Deficit Reduction.Another major threat facing ACA implementation is the bargaining the President must engage in with Congress over the budget, tax legislation, deficit reduction, and the Medicare sustainable growth rate fix. • Although the Democrats made gains in the Senate, the Republicans have retained firm control of the House, and the evisceration of the ACA is likely to be high on their agenda. Republicans could focus on finding cuts in the ACA to fund Medicare physician payment increases, as they have in the past. There is, frankly, little room to cut in the ACA if it is to accomplish its goal of offering affordable health insurance to the uninsured. • If the Administration wants to see this through, they will need to be firm and vigilant in protecting the premium tax credits and Medicaid funding if we are to in fact significantly expand coverage in 2014. • A Technical Corrections Bill? NASMHPD, 2012
ACA Implementation Timeline 2013 • State Notification Regarding Exchanges • Closing the Medicare RX Coverage Gap • Medicare Bundled Payment Pilot Program • Medicaid Coverage of Preventive Services • Medicaid Payments for Primary Care • Itemized Deductions for Medical Expenses • Flexible Spending Account Limits • Medicare Tax Increase NASMHPD, 2012
ACA Implementation Timeline 2013 • Employer Retiree Coverage Subsidy • Tax on Medical Devices • Financial Disclosure • CO-OP Health Insurance Plans • Extension of CHIP • Medicare Disproportionate Share Hospital Payments (DSH) NASMHPD, 2012
Continued Roll Out of the Affordable Care Act • In the near term, HHS is expected to issue a torrent of federal regulations and informal guidance to carry out the law. Without these rules, insurance executives say it is virtually impossible for them to devise the health plans that will be offered in every state through insurance exchanges. • The marketing of those health plans begins in October 2013, for coverage starting Jan. 1, 2014, the date by which the law requires most people to have insurance or pay a tax penalty. But state insurance regulators say they need to start reviewing the new products – for compliance with federal and state laws – much earlier, in the first few months of 2013. • Coverage expansion will be more of a mixed bag. Over the next few months we will see how many states meet deadlines for establishing health insurance exchanges, and whether Governors and legislatures choose to opt into or out of the ACA’s Medicaid expansion following the SCOTUS decision. • Although there is no deadline for states to indicate whether they will expand Medicaid, hospitals and other stakeholders are already lobbying the states to do so. Hospitals will see reimbursement rates trimmed under the health care law, and expanding Medicaid would bring new paying customers to help cover their losses. • Some states are worried about the cost, regardless, and have talked about pursuing a partial expansion instead. NASMHPD, 2012
Continued Roll Out of the Affordable Care Act • As the Administration continues to implement the various provisions of the ACA, it’s worth noting that some aspects are rolling ahead faster than others. • HHS has released rules regarding payment reform pilots (ACOs, shared savings programs, and bundled payments) as well as pay-for-performance initiatives (value-based purchasing, readmissions penalties, etc.). And reductions in Medicare payment updates to providers are expected to go forward on schedule. • The potential misalignment of the timing of payment reductions & coverage expansion only underscores the need for hospitals, health systems, & other providers to continue their efforts to contain long-term costs. NASMHPD, 2012
Looking Over the Horizon • The election is at least in part a referendum on the ACA. Exit polls show that a slim majority of voters support the ACA, and a distinct minority favor full repeal. President Obama did not run away from the ACA in his reelection campaign, and the Republicans continued to attack it, with Governor Romney promising to work toward repeal beginning with his first day in office. • The President’s reelection must be seen as a green light to move forward toward 2014. • With the President reelected and the Democrats strengthening their control of the Senate, it seems possible that less than a year from now millions of Americans will begin enrolling in qualified health plans (QHPs) expecting that premium tax credits will finally become available on January 1, 2014. • Health status underwriting will disappear and pre-existing condition exclusions will be banned. • In most states, Medicaid will become a program that covers all Americans with household incomes below 138 percent of poverty, not just favored categories of the poor. Medicare benefits will continue to improve as the doughnut hole is closed, while Medicare costs will be kept in check. NASMHPD, 2012
Rules Implementing the ACA are Needed for Insurers • Between now and then, however, there is a great deal of work to be done. The exchanges must begin open enrollment on October 1, 2013. By that date, the exchanges must have certified qualified health plans. But before health plans can be certified, they must have their rates and forms approved by the states. • And before that can happen, insurers must determine what plans they will offer and what premiums they will charge. • Yet insurers cannot establish their plans and set their rates until they know a lot more than they do now about the rules they are going to have to play by. If you follow the timeline of these tasks backwards, you get very close to the present. NASMHPD, 2012
Rules Implementing the ACA are Needed for Insurers • Insurers need federal rules right now on the 2014 market reforms – how the guaranteed issue and renewal, preexisting condition exclusions, and age and geographic rating are supposed to work, for example. • Insurers also need more information about how the reinsurance, risk-adjustment, and risk-corridor payment programs are going to work, as this will affect their marketing and pricing strategies. They need to know how medical loss ratios will be calculated, and whether their reserve and surplus requirements will change. • The insurers need to know as soon as possible what the essential health benefits package will be in each state. The states were supposed to have reported to HHS their EHB package by September 30, 2012. • About half the states have chosen a benchmark EHB plan, but the remainder have not. HHS can designate a fallback plan for these states, the largest small group plan in the state, but would prefer that the states designate the benchmark plan. • Reportedly HHS will publish a proposed rule including each state’s benchmark, and states will have an opportunity to comment, essentially getting a second bite at the benchmark decision. NASMHPD, 2012
Rules Implementing the ACA are Needed for States • The states are demanding more guidance on how the federal exchange will partner with the states. • The states must decide by November 16 whether they will operate their own exchange, cooperate with the federal exchange, or allow the federal government to operate the exchange in their state without state involvement. • The NAIC Health Care Reform Regulatory Alternatives Working Group – a group of commissioners from states that have decided against operating a state exchange—recently published a list of questions that they believe must be answered by the federal government about how the federal exchange will interact with the states. • These are serious questions that must be addressed soon by the federal government if it is to hope for state cooperation moving forward. • Behavioral healthcare will experience considerable opportunity as a result of the insurance expansion (13 million enrollees will already have a behavioral health condition) and, at the same time, considerable stress as many behavioral health providers become part of accountable care organizations that operate health homes. NASMHPD, 2012
Status Report on Health Insurance Exchanges • With many states lagging far behind schedule, the Obama Administration said on Nov. 9 that it would extend the deadline for them to submit plans for health insurance exchanges. • If states want to run their own exchanges, HHS said they will have until Dec. 14 to submit applications, or blueprints. • And if states want to run exchanges in partnership with the federal government, she said, they will have until Feb. 15 to file applications. • CBO predicts that 25 million people will obtain coverage through the new insurance exchanges. Most will receive federal subsidies averaging more than $5,000 a year per person to help them pay premiums. NASMHPD, 2012
HHS Continues to Support State Efforts to Build Insurance Exchanges • Secretary Sebelius awarded last month a new round of Affordable Insurance Exchange Establishment Grants. • Arkansas, Colorado, Kentucky, Massachusetts, and Minnesota received awards for Level One Exchange Establishment Grants; these are 1-year grants awarded to states to build Exchanges. D.C. received a Level Two Exchange Establishment Grant, a multi-year grant awarded to states further along in building Exchanges. • A total of 49 states, D.C., and four territories have received grants to begin planning their Exchanges, and 34 states and D.C. have received grants to begin building their Exchanges. • To ensure states have the support and time they need to build an Exchange, states may apply for grants through the end of 2014 and may use funds through the initial start-up year NASMHPD, 2012
The Federal Exchange • The Obama Administration must also move forward with the implementation of the federal exchange. Currently about a third of the states have established exchanges, with a handful more expressing interest in partnering with the federal government. The federal government will need to operate the exchange in all of the states that do not establish their own. This is going to be a massive job. • In establishing the federal exchanges, the Administration faces three major barriers. First, additional funding is probably going to be needed, just at a time when Congress is trying to cut rather than expand federal funding. Second, there is the nagging question of the authority of the federal exchanges to issue premium tax credits. This issue is currently being litigated in Oklahoma. • Third, in the end the states must cooperate with the federal exchange for certain basic functions, such as coordinating Medicaid eligibility determinations and insurance company licensing. The extent to which that cooperation will be forthcoming remains to be seen. NASMHPD, 2012
In the Meantime…Feds Preparing to Sponsor Nation-Wide Health Insurance Plans (Kind of a Public Option) • The Obama Administration will soon take on a new role as the sponsor of at least two nationwide health insurance plans to be operated under contract with the federal government and offered to consumers in every state. • These multistate plans were included in the ACA as a substitute for a pure government-run health insurance program – the public option sought by many liberal Democrats and reviled by Republicans. Supporters of the national plans say they will increase competition in state health insurance markets, many of which are dominated by a handful of companies. • The national plans will compete directly with other private insurers and may have some significant advantages, including a federal seal of approval. Premiums and benefits for the multistate insurance plans will be negotiated by the OPM, the agency that arranges health benefits for federal employees. • Under the Affordable Care Act, at least one of the nationwide plans must be offered by a nonprofit entity. Insurance experts see an obvious candidate for that role: the GEHA. NASMHPD, 2012
Health Insurance Parity Regs • The long-awaited federal regulations on mental health and substance use service parity under the 2008 Wellstone-Domenici legislation and under the ACA will be released in Obama-care-Part 2. • We will need to help implement these regulations in the context of the ACA. • For example, we will need to consider how parity will work when a health benefit is integrated rather than carved out; how parity will work with a performance-adjusted case rate; etc. • A little reflection will suggest that the concept of parity may be different under the ACA than it has been in the past. NASMHPD, 2012
What Can We Expect for Health Care? cont. • Reform Medicare, Medicaid, and Social Security. • As a result of the “fiscal cliff” due to federal deficits and debt, and the threat of sequestration, Obamacare-Part 2 will undertake reform of Medicare, Medicaid, and Social Security. • Only three options are available: alter revenue streams; alter covered populations; or alter benefits. • Solutions offered will be broad-based ideas with potential impact upon everyone—raise the retirement age for Social Security and Medicare enrollment; increase payroll deductions for these programs; remove payment caps; cap annual Medicare and Medicaid benefits, etc. • Because the effort will be designed to apply universally, very careful attention will need to be paid to anticipated impacts on persons with mental illness, substance use, and I/DD conditions. NASMHPD, 2012
Update on ACA Essential Health Benefits • NO regs yet but it’s crunch time for states that are working to select their benchmark plans for essential health benefits. Deadline passed for a decision to be submitted to HHS officials. • According to our information, 16 states have identified their proposed benchmark plans that will be the models for individual and small-group insurance coverage in each state's health insurance exchange. Another 17 have identified their potential benchmarks plans so the final tally of states that submit proposed benchmarks to HHS could still rise substantially. • States that have picked benchmark plans are: Arkansas, California, Colorado, Connecticut, Delaware, Maryland, Michigan, Mississippi, New Hampshire, Oregon, Rhode Island, Utah, Vermont, Virginia, Washington, and the District of Columbia. • HHS officials also told states the deadline to pick a plan by the end of the third quarter of the year was a "soft" one since it was not set out as a formal regulation, according to a letter sent to some state officials. Appears that HHS will begin reaching out to states that have not submitted benchmarks to discuss a default plan. NASMHPD, 2012
Update on Electronic Health Records • Republican House leaders want federal officials to suspend payments to hospitals and doctors who switch from paper to electronic health records, arguing the program may be wasting billions of tax dollars and doing little to improve the quality of medical care. • In an Oct. 4 letter to HHS Secretary Sebelius, the leaders suggested that $10 billion spent so far on the program has failed to ensure that the digital systems can share medical information, a key goal of the effort. • The letter urges Sec. Sebelius to “change the course of direction” of the H.I.T. incentive program to require that doctors and hospitals receiving tax money get digital systems that can “talk with one another.” The letter urges Sec. Sebelius to suspend payments under the program until rules are written requiring that the systems share information. • Obama Administration expects to spend more than $30 billion to help doctors and hospitals purchase appropriate technology and use it to improve health care. More than 50% of the nation’s hospitals have received some payments, and so far more than $10 billion has been spent. About one-half of the doctors now billing Medicare use digital records. NASMHPD, 2012
The Ever-Approaching “Fiscal Cliff” • With the election over, both the President and Congress have turned their immediate attention to looming deadlines on major issues including the expiring tax cuts and automatic spending cuts under the Sequester, and the Medicare physician payment fix. • President Obama, Senate Majority Leader Reid and House Speaker Boehner have all signaled that they would like to reach an agreement before Congress adjourns near Christmas on the general contours or comprehensive framework of the FY 2013 budget and budget deficit reduction legislation, including reductions in spending and changes to the tax code. • Speaker Boehner has been resistant to any effort to make major tax or spending changes in the lame-duck session of Congress. • It is not clear if the leaders & parties can reach agreement on the framework – we may witness more brinkmanship before they adjourn in December. NASMHPD, 2012
Kicking the Can Down the Road (But With a Purpose?) • Either way, late this year or very early next year the current law (the Sequester is scheduled to kick in on Jan. 2) will be extended at least through July to give the new Congress time to craft the large package of tax, entitlement and deficit-reduction reforms we know will be on the table. • Final passage of this measure would be targeted for late 2013. • Medicare and Medicaid likely will be part of the deficit discussion, and formerly untouchable elements of the Medicare program (e.g., changes to beneficiary cost-sharing) will likely be discussed alongside additional provider payment cuts. • Instead the lame-duck session will be used as a legislative vehicle to develop a short-term deal to delay the year-end fiscal cliff. Key principals would supports a short-term “bridge” that would extend all of the tax rates for one year and buy more time to overhaul the federal tax code next year, e.g., closing loopholes not raising the rates individuals pay on their wages. NASMHPD, 2012
Reality is Setting in on Both Sides(Pushed by CEOs and Key Experts) • According to many economists and federal budget experts, the budget deficit cannot rise faster than the economy indefinitely without causing economic and financial problems – but too much deficit reduction, too soon, could derail the economic recovery. So policymakers must steer a course between these two unacceptable outcomes as they confront the twin challenges of giving the recovery a boost in the short term while stabilizing the debt over the longer term. • These challenges lie at the heart of upcoming negotiations among President Obama, the Republican-controlled House, and the Democratic-led Senate over how to address the "fiscal cliff“. • The Congressional Budget Office estimates that letting all these changes take effect and remain in place would likely cause a recession in the first half of 2013. If, by contrast, policymakers change the laws and extend all current policies for a prolonged period, debt held by the public would continue rising much faster than gross domestic product, thus raising economic and financial risks. • Policymakers could achieve a better outcome than either of these alternatives by enacting enough deficit reduction to stabilize the debt-to-GDP ratio over the next decade but structure it so that the cuts are not fully phased in until the economy is stronger. NASMHPD, 2012
The Fiscal Cliff:Grand Bargain Issues • During the 2011 negotiations between President Obama and House Speaker Boehner, the House GOP leadership lobbied for significant reforms. Democrats agreed to make cuts around the edges but were less than amenable to large-scale changes. Repeatedly, they told GOP lawmakers that they would consider more ambitious reforms only if increased revenues were also on the table. • To achieve significant and long-term savings, they proposed raising the Medicare eligibility age from 65 to 67, means-testing benefits further, using systematic research to prioritize effective treatments and increasing premiums on seniors. • The White House did give some indication that it would be willing to broker a compromise on Medicare. During his talks with House Speaker Boehner, President Obama allowed that he could be open to raising the eligibility age to 67 and to increasing premiums for those seniors in the highest income brackets. • On Medicaid, too, Republicans asked for serious structural reforms, and Democrats again asked for revenues before cutting back on benefits. NASMHPD, 2012
Sizing Up the Fiscal Cliff: Update on the Cost of Expiring Tax Cuts and Federal Budget Deficit Reduction (in billions) • Bush Era Tax Cut (below $250k income) = $198 billion • Alternative Minimum Tax Patch = $120 • Payroll Tax Holiday = $115 • Automatic Spending Cuts (Sequester) = $110 • Bush Era Tax Cut (above $250k income) = $83 • Emergency Unemployment Insurance = $40 • Affordable Care Act Implementation = $20 • Medicare Doc Fix = $20 • Tax Extenders = $20 • Bonus Depreciation = $12 • Total = $738 billion (on or around January 1, 2013 -- or 4.6% of GDP NASMHPD, 2012
Driving Toward the Fiscal Cliff • Nothing substantive will occur before the election as there is little political will to make tough decisions. • Hellacious lame duck session (looking at a 6-week period) is in store to deal with the expiration of the Bush tax cuts, “extenders” package expires (e.g., unemployment benefits) and the Sequester and major interest groups fighting over a shrinking pie. • Sequester could be a knockout punch for key health care programs as several federal agencies, on average, have already incurred 4-5% cuts since 2010: • SAMHSA = 8.2% cut (possibly 12-14%?) • HRSA = 8.2% cut • NIH = 8.2% cut • NASMHPD working with NDD Coalition. Key message “Cuts alone will not stop federal budget deficit and debt problems – need balanced approach.” NASMHPD, 2012
Mental Health Under the Sequester Assuming a 10% cut to (medium estimate) all SAMHSA programs and other public health activities and research, we estimate that under sequestration: • About 700,000 individuals with mental health conditions, will lose critical employment and housing assistance, case management services, and school-based supports. • Over 1.1 million children and adults will be at risk of losing access to any type of public mental health support. • More than 320,000 children will miss out on coordinated mental health services, early intervention and prevention programming, and other suicide prevention services. • Nearly 170,000 fewer individuals will be admitted to substance use treatment programs. Do policymakers want to go over this cliff?
Mental Health and the Sequester • At the beginning of the budget season, SAMHSA was told to submit a budget proposal to OMB reflecting a net 5% spending reduction. SAMHSA proposed a 2% spending reduction in FY 2014 instead and OMB agreed. At this juncture, SAMHSA is awaiting their OMB pass back. • In defending both block grants during their OMB presentations, SAMHSA leadership team basically presented a series of arguments about why the MHBG and SAPT Block Grants remain relevant in the aftermath of ACA implementation. • There is wide existing treatment gap that stagnant funding of the block grants has exacerbated. Many persons with serious mental illnesses and addiction disorders will remain without health insurance despite the ACA coverage expansions. Many services now covered by the block grants will not be reimbursed by either Medicaid or the mental health/addiction benefit in the state exchanges (namely, peer support services and 30-day residential treatment for addiction disorders). • Apparently, the lower levels of OMB have bought these arguments. NASMHPD, 2012
Mental Health Under the Sequester • House and Senate appropriators are looking closely at rolling an FY 2013 Continuing Resolution into the budget package the cancels the so-called fiscal cliff (and thereby extending government funding through the end of Sept). Under such a scenario, the basic fiscal operating principal is that federal government funding – including SAMHSA appropriations -- would largely be frozen at FY 2012 levels with a few fixes/adjustments thrown in. • In practice, that larger settlement if it materialize, appears to jeopardize the $20 million increase in FY 2013 funding we secured for the MHBG in the Senate bill, although SAMHSA’s top line budget number across mental health and addiction programs is better off under this scenario. • We have been encouraged by Sen Harkin’s subcommittee staff to begin lobbying outgoing Chairman Rehberg and Rep. DeLauro on the SAMHSA budget emphasizing a law enforcement angle. NASMHPD, 2012
The Fiscal Cliff “Mitigation” Option • Obama Administration could blunt the economic harm of the fiscal cliff if negotiations fall apart by using its unilateral powers over spending and taxes by freezing how much in taxes is taken out of payroll checks. • Also soften the blow from dramatic federal spending by shifting available $$ toward paying immediate costs – such as government employee salaries – rather than saving for construction costs. • The goal is to buy time to reach a new budget deal. NASMHPD, 2012
Long Term Federal Deficit Reduction • Gang of 6 Plus 2 in talks of long-term deficit reduction running into the trillions of dollars using the unsuccessful (so far) Simpson-Bowles Commission as the eventual basis of compromise: Tax Increases Along Side Spending Cuts. • Judged against the standards of long-standing health policy, Simpson-Bowles would bring dramatic change – taxation of health benefits, a cap on overall health care spending by the federal government, an end to Medigap coverage in its current form, and possibly a premium-support based overhaul of Medicare. • Simpson-Bowles would institute a never-attempted change: Long-term global budget for total federal health care spending. Starting in 2020, it would hold yearly growth in such spending to GDP plus 1 percent. The cap would take into account federal spending for Medicare, Medicaid, CHIP, FEHBP, TRICARE, insurance exchange subsidies and the cost of the remaining tax exclusion for health care. • If growth exceeded budget target, the President and Congress would have to act and would likely need to consider major structural reforms to the health care system beyond ACA. NASMHPD, 2012
Key Components of the New Massachusetts Law to Constrain Health Care Costs • Sets targets for limiting annual increases in health care spending to the rate of growth in the GSP for 2013–2017, 0.5 percentage point less than the GSP growth rate for 2018–2022, & the GSP growth rate again for 2023 and beyond. • Requires Medicaid, state employee health plans, and other state-funded programs to adopt alternative payment models (including shared savings programs, global payments, and bundled payments) to replace traditional fee-for-service payments. • Promotes establishment and certification of ACOs, and medical homes to improve coordination of care & access to preventive and PC services, & authorizes contracting preferences for these organizations in insurance programs. • Establishes health policy commission as independent public entity to oversee cost-growth targets & monitor new delivery/payment models. • Creates special commission to report on variations in provider prices. NASMHPD, 2012
Key Components of the New Massachusetts Law to Constrain Health Care Costs, cont. • Requires providers that exceed the cost-growth benchmark to file and implement a performance-improvement plan, with potential penalty up to $500,000 for failure to comply. • Enhances transparency through expanded public reporting of quality of care and prices using a standard set of measures for common health care services on a public website. • Addresses medical malpractice with a 182-day cooling-off period before patients can file a lawsuit, and makes providers' apologies to patients inadmissible in malpractice proceedings. • Establishes $135 million fund to support financially distressed hospitals. • Establishes Massachusetts eHealth Institute with $30 million fund to accelerate adoption of interoperable electronic health records. • Authorizes $60 million over 4 years for wellness and preventive health programs and an annual tax credit up to $10,000 for businesses that create workplace wellness programs. • Covers expected costs of new law ($225 million) through one-time surcharges on health insurers ($165 million) and large hospitals ($60 million). NASMHPD, 2012
Medicare Coverage Decision • A proposed settlement of a national class-action lawsuit, filed October 16 in U.S. District Court in Vermont, says the government will revise its Medicare manual to make benefits available when care would only "maintain the patient's current condition or ... prevent or slow further deterioration". It is expected that the Vermont judge handling the case will sign off on the federal agreement. • The Obama Administration has agreed to relax Medicare's requirements for skilled nursing and home health care, allowing beneficiaries to qualify for benefits even if their conditions are not expected to improve, according to court documents. • The new language would ensure broader availability of Medicare coverage for skilled nursing, home health and outpatient care and mark a significant departure from longstanding practices that insist on evidence of medical improvement to sustain coverage. • The settlement will eliminate a major barrier to care for thousands of people with chronic or degenerative conditions such as psychiatric disorders, multiple sclerosis, and spinal cord injuries. Until this agreement, individuals and their families have often been left to choose between the high cost of skilled nursing and home care or the prospect of managing the care of family members on their own. Beneficiaries have frequently been denied Medicare coverage. NASMHPD, 2012
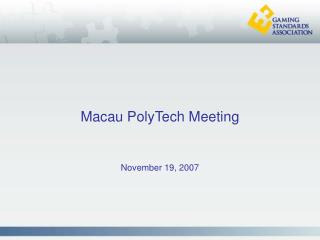
Figure 1 The Waterfall Cascading Impact of Medicaid Expansion on State Budgets (In Billions of Dollars) 2014-2023 State Budget Gains from Increased Federal Spending on Existing Medicaid Enrollees1 $66 State Budget Gains from Increased Federal Spending on Ending Medicaid Coverage for Adults > 138% of FPL Covered by Waivers2 $69 State Gains From Reduced Spending on Uncompen- sated Care $85 State Gains from Increased Federal Spending on BH Services $39 State Gains in Out-years of Medicaid Expansion From 2020-23 $76 State Gains from Better Care Coordination of Dual Eligibles $34 State Gains on Medicaid Drug Rebates $8 = $377 Billion in Savings - $73 Billion in Implementation Costs ____________________________ $304 Billion in Total State Savings • All budget gains related to Medicaid Expansion are for acute care costs only (e.g., physician costs not included). • Budget gains due to maintenance of effort, ending eligibility for special categories of adults (e.g., individuals with breast cancer), and shifting costs to insurance exchanges for “Medically Needy” adults.
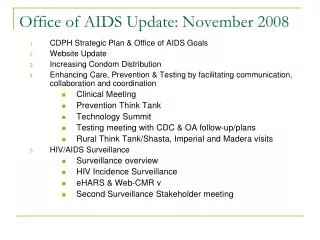
Figure 2 The Waterfall Cascading Impact of Medicaid Expansion on State Economies Increased State Revenue From Taxes on Insurance Premiums Increased Federal Dollars on Behalf of New Enrollees Affecting Providers Creation of New Jobs Associated with Delivering Services Increased Income Associated with Delivering Services Increased Purchases Associated with Carrying Out Health Care Services Influx of New Federal Dollars Benefitting Other Businesses and Industries Indirectly Induces Changes in Household Consumption and Tax Collection
Medicaid Expansion is a Great Buy for States • The Medicaid expansion under the ACA can serve as a three-pronged major “waterfall cascading” effect on state budgets, state-wide economies and for people without health insurance coverage. • Several States are reassessing their positions on whether to choose to opt in to the Medicaid expansion after indicating they would not opt in. SBHAs, where possible, can be active in promoting the major impacts of the expansion for people with BH conditions and the financial benefits for their state. • States should expand Medicaid eligibility, beginning January 1, 2014 at the latest (to obtain the 100% match) for all individuals with incomes below 138 percent of the FPL, and especially for people with mental illness. • States can only offer so many services for people with serious mental illness. The opportunity to improve this situation substantially could be lost if a state fails to choose to opt in to the Medicaid expansion. NASMHPD, 2012
Behavioral Health Challenges • ACA Implementation - Exchanges - Medicaid Expansion - Essential Health Benefits - Workforce Issues • The Fiscal Cliff • Ongoing Budget Battles NASMHPD, 2012
Questions&For more information, please contact me at joel.miller@nasmhpd.org, or at 703-739-9333 NASMHPD, 2012