Download
1 / 27
630 likes | 2.17k Views
Menstrual Cycle Disorders. Karen Estrella H. Pediatric PGY -2 SBH Nov/2010. Objetives. Introduction Normal physiology Definitions Menstrual Cycle disorders Amenorrhea Dysfunctional Uterine Bleeding Dysmenorrhea. Introduction. Menarche: Median age: 12.7 yrs

E N D
Menstrual Cycle Disorders Karen Estrella H. Pediatric PGY-2 SBH Nov/2010
Objetives • Introduction • Normal physiology • Definitions • Menstrual Cycle disorders • Amenorrhea • Dysfunctional Uterine Bleeding • Dysmenorrhea
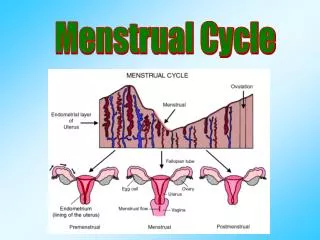
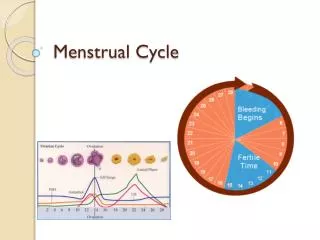
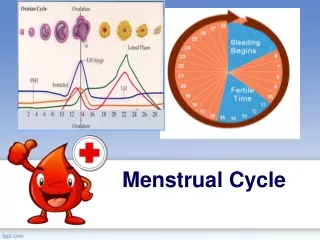
Introduction • Menarche: • Median age: 12.7 yrs • African-american earlier than Caucasian • 2-2.5yrs after breast development • Anovulatory cycles: 1st 1-2yrs of onset (55-82%) • For 5 yrs (10-20%) • Duration: • Between 21 and 35 days (mode: 28) • Lasting: 3-7days • Blood lost: 30-40ml
Definitions • Amenorrhea: • Primary: absence of menarche by age 16 in the presence of normal pubertal development (Tanner 4-5) • Or: lack of menses by age 14 in absence of pubertal development • Secondary: absence of 3 consecutive menstrual cycles or 6 months of amenorrhea • Menorrhagia: normal intervals with excessive flow • Cycles more than 8days, > 80ml • Metrorrhagia: irregular intervals with excessive flow • Oligomenorrhea: menstruation ocurring more than every 35 days to 6 months
Amenorrhea • Classification: • With pubertal delay • With normal pubertal development • Genital abnormalities • Hyperandrogenic anovulation
Amenorrhea1. With pubertal delay • Hypergonadotropic hypogonadism • OVARIAN FAILURE • Turner • XY gonadal dysgenesis • Autoinmmune oophoritis • Exposure to chemo or RT(alkylating) • 17 alpha hydroxylase deficiency Elevated FSH B A
Amenorrhea1. With pubertal delayB. Hypogonatropic hypogonadism PITUITARY: • Adenoma • Prolactinoma • Craniopharyngioma • Hemochromatosis • Hypothyroidism • Breast stimulation • Sx • Phenothiazines, opiates • (-PRL inhibitor factor) HYPOTHALAMIC: • Suppresion: • Stress • Malnourishment • Wt loss < 15% of ideal body wt • Strenous exercise • Body fat < 22% • If prior to menarche, each yr of training delays onset by 5 months • Prader-Willi • Kallman • Migration olfatory and GnRH neurons) • Low or normal FSH
Amenorrhea2. with normal pubertal development • Pregnancy • Chronic diseases • Exc IBD, DM, hypothyroidism, anorexia • Use of hormonal contraceptive • Progestational effect • Uterine synechiae (Asherman sd) • Sheehan sd.
Amenorrhea3. Genital tract abnormalities • Outflow tract-related: • Imperforate hymen • Transverse vaginal septum • Agenesis of the vagina, uterus: • Mullerian Agenesis: breasts, (+) pubic and axillary hair • Testicular feminization (x-linked defect androgen receptor): breast, (-) pubic axillary hair
Amenorrhea4. Hyperandrogenic anovulation • Hirsutism, acne, rarely clitoromegaly To be r/o: • PCOS (polycystic ovarian syndrome) • Most common • Ovarian and adrenal tumor or adrenal enzyme deficiency • Obesity
Primary amenorrhea Presence of breasts TSH PRL MRI brain testosterone Surgery Enzymatic defect Hormone replacement
Secondary amenorrhea >100ng/ml DHEAS: > 700ng/ml Testosterone >90ug/ml Abd-pelvic MRI 17OH progesterone Asherman • Hirsutism: spirinolactone 50mg po TID
Evaluation: Secondary amenorrhea • Progesterone challenge test: • Oral medroxyprogesterone acetate for 5-10 mg QD for 5-10 days), or IM 200mg x1. • POSITIVE TEST: withdrawal bleeding 2-7 days after • +uterus • +estrogen stimulation: ovaries ok • Estrogen-progesterone challenge test: • Oral conjugated estrogen (1.25 mg) or 2 mg estradiolqd for days 1 through 21 with oral medroxyprogesterone acetate (10 mg) on days 17 through 21. • POSITIVE TEST: withdrawal bleeding 2-7 days after • +uterus • Insufficient estrogen stimulation
Dysfunctional Uterine Bleeding • Prolonged # of days of bleeding or excessive bleeding • Most common: anovulation • the lack of progesterone secretion increases risk of endometrial hyperplasia High estrogen levels Bleeding is prolonged, irregular and sometimes profuse Adolescents Obese
DUB: Differential dx • Pregnancy • STD’s • PID • Foreign bodies • Cervical neoplasia • Coagulation defect: vWF
Dysmenorrhea(painful menses) Primary: • Decrease of progesterone levels al end of luteal phase: lysosomal membranes are unstable::::release enzymes formation: Prostaglandins Keep increasing during luteal and menstrual phases Uterine hypercontractibility Tissue ischemia Nerve hypersensitivity (just before or 1st days of menses) Secondary: • Associated with pelvic pathology: • Endometriosis • Miomas • PID • STD • Genital tract obstruction (Later age, Menorrhagia, Dyspareunia, Pain with defecation, worsening with every cycle or mid-cycle, symptoms that persist after menses have finished)
Dysmenorrhea: Treatment • Inhibiting prostaglandin synthesis: • Ibuprofen: 400-600mg po q4-6hrs • Naproxen 500mg load then 250mg po q6-8hrs • Started on 1st day of bleeding • Prevent ovulation and decrease endometrial growth • Oral contraceptives • 30-35mcg combined estrogen-progestin x4-6months • Laparoscopy
References • http://pedsinreview.aappublications.org/cgi/reprint/13/2/43?maxtoshow=&hits=10&RESULTFORMAT=&fulltext=menstrual+disorders&searchid=1&FIRSTINDEX=0&sortspec=relevance&resourcetype=HWCIT • http://www.aafp.org/afp/2006/0415/p1374.html • http://www.wrongdiagnosis.com/symptoms/missed_period/book-causes-10a.htm • http://pedsinreview.aappublications.org/cgi/reprint/18/1/17?maxtoshow=&hits=10&RESULTFORMAT=&fulltext=menstrual+disorders&searchid=1&FIRSTINDEX=0&sortspec=relevance&resourcetype=HWCIT • http://pedsinreview.aappublications.org/cgi/reprint/13/3/83?maxtoshow=&hits=10&RESULTFORMAT=&fulltext=menstrual+disorders&searchid=1&FIRSTINDEX=0&sortspec=relevance&resourcetype=HWCIT • http://courses.washington.edu/conj/bess/reproductive/pcos2.png • http://img.medscape.com/article/720/869/720869-box2.jpg • http://www.theberries.ca/archives/dub1.html • http://www.medicine4faith.net/wp-content/uploads/2010/08/ovarCon.jpg