Download
1 / 69
760 likes | 1.04k Views
The Treatment of Obesity. Proven approaches to treating obesity and its associated co-morbidities. DSL#12-1303. This promotional education activity is brought to you by Ethicon and is not certified for continuing medical education. XXX is a paid consultant of Ethicon. Presentation Topics.

E N D
The Treatment of Obesity Proven approaches to treating obesity and its associated co-morbidities DSL#12-1303
This promotional education activity is brought to you by Ethicon and is not certified for continuing medical education. XXX is a paid consultant of Ethicon.
Presentation Topics • What is obesity? • Obesity treatment options • Recent clinical evidence • Obesity patient management
Obesity is a complex, multi-factorial, chronic metabolic disease Obesity involves the following factors: American Obesity Association. Fact Sheet: Obesity in the U.S. May 2, 2005. http://www.obesity.org
A contributing factor to obesity is the body’s metabolic “set point” Sumithran P, Prendergast, LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011; 365:1597-1604.
Hormones play a significant role in controlling weight Cummings DE, Weigle DS, Frayo RS et al. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med. 2002; 346(21): 1623-30. Cummings DE, Schwartz M. Genetics and pathyphysiology of human obesity. Annu Rev Med 2003; 54:453-71.
The National Institute of Health uses BMI to define obesity • Body mass index (BMI) is: • a measure of body fat based on height and weight. • Morbid obesity is: • a multi-factorial disease of excess fat storage (40+ BMI) and associated diseases of other systems • lifelong and progressive. Vorvick LJ. Body Mass Index. MedlinePlus. Accessed October 9, 2012 from http://www.nlm.nih.gov/medlineplus/ency/article/007196.htm
According to NIH guidelines, here is what obesity looks like* Normal Weight (BMI 19 to 24.9) Overweight(BMI 25 to 29.9) Obese (Class I)(BMI 30 to 34.9) Obese (Class II)(BMI 35 to 39.9 ) Morbidly Obese(BMI 40 or more) 130 pounds BMI 22 152 pounds BMI 26 175 pounds BMI 30 205 pounds BMI 35 234 pounds BMI 40 *For a 5’4” female Vorvick LJ. Body Mass Index. MedlinePlus. Accessed October 9, 2012 from http://www.nlm.nih.gov/medlineplus/ency/article/007196.htm and National Heart Lung Blood Institute. Classification of Overweight and Obesity by BMI, Waist Circumference, and Associated Disease Risks. Accessed October 9, 2012 from http://www.nhlbi.nih.gov/health/public/heart/obesity/lose_wt/bmi_dis.htm
One third of the U.S. adult population is considered obese and the number is growing % of the population that is obese by state 1990 2010 75 million adult Americans are considered obese Ogden CL, Carroll MD, Kit BK et al. Prevalence of obesity in the United States, 2009-2010. NCHS Data Brief 2012; 82 and Centers for Disease Control and Prevention. US Obesity Trends, trends by state 1985-2010
There is a significant economic impact of obesity • $168 billion is the estimated US annual medical cost of obesity1 • There is 50% higher per capita medical spending on obese patients than for normal weight individuals1 • There is an 80% higher prescription drug spending for the obese patient than for normal weight individuals2 • 16.5% of national health expenditures are spent treating obesity-related illness1 Obesity is an expensive disease. 1. Cawley, J, Meyerhoefer, C. The Medical Care Costs of Obesity: An Instrumental Variables Approach. National Bureau of Economic Research. October 2010. 2. Finkelstein EA, Trogdon JG, Cohen JW et al. Annual medical spending attributable to obesity: Payer- and service-specific estimates. Health Affairs 2009; 28(5):w822-w831.
There are significant co-morbidities associated with obesity Depression Pulmonary disease abnormal PFTs obstructive sleep apnea hypoventilation syndrome Stroke GERD Cardio/Metabolic Syndrome diabetes dyslipidemia hypertension metabolic syndrome Nonalcoholic fatty liver disease steatosis steatohepatitis cirrhosis Gallbladder disease Severe pancreatitis Gynecologic abnormalities abnormal menses infertility polycystic ovarian syndrome stress incontinence Cancer breast, uterus, cervix, colon, esophagus, pancreas kidney, prostate Osteoarthritis Phlebitis venous stasis Skin Premature Death Gout References at end of presentation
As a patient’s BMI rises, so does the prevalence of co-morbid conditions Prevalence of Significant Morbidities per Weight Stommel M, Schoenborn CA. Variations in BMI and prevalence of health risks in diverse racial and ethnic populations. Obesity 2010; 18(9):1821-1826.
Obesity has serious consequences • Life expectancy decreases as BMI increases • For people with obesity, there is a 33% to 179% higher risk of mortality Graph represents years of life lost for white men. Allison DB, Fontaine KR, Manson JE et al. Annual deaths attributable to obesity in the United States. 1999; 282(16):1530-1538. Fontaine KR, Redden DT, Wang C et al. Years of life lost due to obesity. JAMA 2003;289:187.
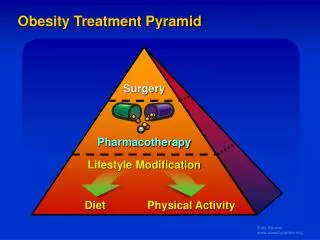
The recommended treatment for obesity depends on the severity of the disease National Institutes of Health. The practical guide: Identification, evaluation, and treatment of overweight and obesity in adults. NIH Publication Number 00-4084; 2000.
Lifestyle Modifications • Caloric intake should be reduced by 500 to 1,000 calories per day (kcal/day) from the current level. • Daily food logs for 4-6 weeks • Weekly weigh-in • Increased physical activity • Water intake • Behavior modification
Lifestyle Modifications • Comparison of weight loss/behavior programs: Atkins®, Zone, Weight Watchers®, and Ornish Diets According to the Swedish Obesity Study 20 year data published in JAMA, patients lost 1% with diet and lifestyle changes. Dansinger ML, Gleason JI, Griffith JL, et al. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease reduction. JAMA 2005;293(1)43-53. Sjostrom L, Peltonen M, Jacobson P et al. Bariatric surgery and long-term cardiovascular events. NEJM 2012; 307(1):56-65. Atkins is a registered trademark of Atkins Nutritionals, Inc.Weight Watchers is a registered trademark of Weight Watchers International, Inc.
Pharmacotherapy: Medications for Weight Loss • For patients with: • BMI ≥ 27 with co-morbidities or • BMI ≥ 30 without co-morbidities • There are 5 drugs currently available for patients. • Alli® • Xenical® • Adipex® • Qsymia™ • Belviq® Trademarks are the property of their respective owners.
Pharmacotherapy Xenical Prescribing Information. 2. Alli product label. 3. ePocrates–Adipex-P monograph; Li Z, MaglioneM, TuW et al. Meta-analysis: Pharmacologic Treatment of Obesity. Ann Intern Med. 2005;142:532-546. 4. QsymiaPirescribing Information 5. Belviq Prescribing Information.
Bariatric & Metabolic Surgery: • For patients with: • BMI ≥ 35 with co-morbidities or • BMI ≥ 40 without co-morbidities • Provides medically significant sustained weight loss • Involves alteration of the GI tract that affects cellular and molecular signaling and leads to a physiologic improvement in energy balance, nutrient utilization, and metabolic disorders. • Examined in many clinical studies for effects on weight and co-morbidities
Comparison of surgical treatment options Surgery is Currently the Most Effective Treatment for Morbid Obesity Average Weight Loss from baseline; meta-analysis of various studies up to 4 years in length. 1. Phillips E, Ponce J, Cunneen SA, et al. Safety and effectiveness of REALIZE® adjustable gastric band: 3-year prospective study in the United States. SurgObesRel Dis. 2009; 5:588-597. P<0.001 2. Fischer L, Hildebrandt C, Bruckner T, Kenngott H, Linke GR, Gehrig T, Büchler MW, Müller-Stich BP. Excessive weight loss after sleeve gastrectomy: a systematic review. Obes Surg. 2012 May;22(5):721-31. 3. O’Brien PE, McPhail T, Chaston TB, et al. Systematic review of medium-term weight loss after bariatric operations. Obes Surg. 2006; 16(8):1032-1040.
Major medical societies are advocating for bariatric surgery “It is clear that obesity surgery today offers the only effective long-term treatment option for the severely obese patient.” - American Heart Association (AHA), 2011 “Bariatric surgery should be considered for adults with BMI ≥ 35 kg/m2 and type 2 diabetes, especially if the diabetes is difficult to control with lifestyle and pharmacologic therapy.” - ADA “The Standards of Medical Care in Diabetes,” 2009 “Weight-loss surgery is the most effective treatment for morbid obesity producing durable weight loss, improvement or remission of co-morbid conditions, and longer life.” - Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), 2009 1 Poirer.P, Cornier M-A, Mazzone T. Bariatric surgery and cardiovascular risk factors: A scientific statement from the American Heart Association.Circulation 2011;123:1683-1701.l 2 American Diabetes Association. Standards of medical care in diabetes – 2009. Diabetes Care 2009; 32 (S1): S13-S61 3 SAGES Guidelines Committee. SAGES guideline for clinical application of laparoscopic bariatric surgery. SurgEndosc 2008 Oct;22(10):2281-300
Treatments Prescribed for Morbid Obesity Avidor Y, Still CD, Brunner M, et al. Primary care and subspecialty management of morbid obesity: referral patterns for bariatric surgery. SurgObesRelat Dis. 2007;3(3):392-407
Continuum of care for the obese patient There are many healthcare professionals that must work together to identify the right time for the right treatment. .* From Janssen
Bariatric Surgery Procedure Types A laparoscopic approach for bariatric surgery is performed ~90% of the time. Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2008. ObesSurg 2009; 19:1605-1611.
Bariatric surgery – most common procedures Roux-en-Y Gastric Bypass Sleeve Gastrectomy Adjustable Gastric Banding Bypass a portion of the small intestine and create a 15-30cc stomach pouch Re-sect approximately three-fourths of the stomach Place implantable device around upper most part of stomach ~245,000 procedures annually (US)
There are significant co-morbidity improvements associated with bariatric surgery Depression* 47% reduced Obstructive sleep apnea 45% to 76% resolved Migraines* 46% improved Diabetes 25% to 66% controlled Hypertension 42% to 66% resolved Asthma 39% improved Urinary stress incontinence* 50% resolved Nonalcoholic fatty liver disease 37% resolution of steatosis Osteoarthritis* /Degenerative joint disease 41% resolved References at end of presentation. * Study population predominantly female.
90-Day Adverse Event Rates by Procedure* *When performed at a Bariatric Surgery Center of Excellence Serious events include death, anastomotic leakage, cardiac arrest, deep vein thrombosis, evisceration, heart failure, liver failure, multi-system organ failure, myocardial infarction, pneumothorax, pulmonary embolism, renal failure, respiratory failure, sepsis, stroke, systemic inflammatory response syndrome, and bleeding requiring blood transfusion. Does not include non-serious events such as nausea/vomiting, dehydration, and atelectasis. SRC BOLD Report: Summary of Key Statistics Prepared for SRC’s Strategic Alliance Partners. March 2010. Data is reported on 80,157 research-consented patients who have had a surgery entered in BOLD from June 2007 through Sept 22, 2009. All patients with data in BOLD have had their bariatric surgery performed by a surgeon participating in SRC’s Bariatric Surgery Center of Excellence (BSCOE) program.
CMS: Inpatient Discharge Data (2010)Morbidity & mortality rates of gastric bypass are similar to other common procedures Source: Direct Research, LLC, Center for Medicare and Medicaid Services, FY 2010 MedPAR, Medicare Fee-for-Service Inpatient Discharges with Selected Procedures
Bariatric Surgery: Benefits vs. Risks • Benefits: • Highest level of excess weight loss • Co-morbidity resolution or reduction • Reduction in mortality • Risks: • General risks of surgery • Band erosion / slippage / leak / malfunction • Esophageal spasm/reflux or esophageal/stomach inflammation • Gastric perforation • Outlet obstruction Note: Lists are not exhaustive. Risks are in addition to the general risks of surgery. Patient weight, age and medical history play a significant role in determining specific risks.
Recent Clinical EvidenceBariatric Surgery and Medication Usage
STAMPEDE Surgical treatment and medications achieved glycemic control in more patients than medical therapy alone. Schauer PR, Kashyap SR, Wolski K, et al. Bariatric Surgery versus Intensive Medical Therapy in Obese Patients with Diabetes. N Engl J Med. 2012; 366:1567-1576. Study supported by a grant from Ethicon.
STAMPEDE results Surgical treatment and medications achieved glycemic control of HbA1c < 6.0% in more patients than medical therapy alone Significantly more diabetic patients achieved glycemic control following bariatric surgery * ** Medical Therapy + Gastric Bypass *p=0.002 Medical Therapy + Sleeve Gastrectomy **p=0.008 Medical Therapy Glycemic control: HbA1c < 6.0% with or without diabetes medications, 12 mo after randomization. Figures adapted from study data.
STAMPEDE results Surgical treatment and medications achieved glycemic control of HbA1c < 7.0% in more patients than medical therapy alone Significantly more diabetic patients achieved glycemic control following bariatric surgery * * ** Medical Therapy + Gastric Bypass *p<0.001 Medical Therapy + Sleeve Gastrectomy **p<0.001 Medical Therapy Glycemic control: HbA1c < 7.0% without diabetes medications, 12 mo after randomization. Figures adapted from study data.
Mingrone Bariatric surgery resulted in better glucose control than did medical therapy Mingrone, G, et. al. Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes, N Engl J Med 2012, March 26, [Epub ahead of print]
Mingrone – ResultsGlycatedHemoglobin Levels during 2 Years of Follow-up Mingrone, G, et. al. Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes, N Engl J Med 2012, March 26, [Epub ahead of print]
Buchwald(systematic review) T2DM resolved or improved in 87% of patients following bariatric surgery
Buchwald: Systematic Review & Meta-Analysis (2009)T2DM resolved or improved in 87% of patients following bariatric surgery 99% • Systematic review & meta-analysis reviewing 621 studies including 135,246 patients • Overall, T2DM 87% resolved or improved (78% resolved) for patients after bariatric surgery 87% 87% 85% 81% Total Buchwald H, Estok R, Farbach K, et al. Weight and Type 2 Diabetes after Bariatric Surgery: Systematic Review and Meta-analysis. Am J Med. 2009;122(3):248-256. Figure adapted from source data. Data included includes 621 studies with 888 treatment arms & 135,246 patients; 103 treatment arms with 3188 patients reported on resolution of diabetes. Resolution based on clinical and laboratory manifestations of diabetes resolved (off diabetes medications with normal fasting blood glucose [<100 mg/dL] or HbA1c [≤6%]),
Klein(3 year matched cohort analysis) 46% fewer T2DM related claims for patients with bariatric surgery
Klein: 3-Year Matched Cohort Analysis (2011) 46% fewer T2DM-related claims for patients following bariatric surgery • 56% fewer diabetes prescriptions were filled for bariatric surgery patients. • There was a significantly lower supply cost in diabetes medication for surgery patients. Source: Klein S, Ghosh A, Cremieux PY, Eapen S, McGavock TJ. Economic impact of the clinical benefits of bariatric surgery in diabetes patients with BMI ≥35 kg/m2. Obesity. 2011;19:581-587.
Segal(AHRQ 1 – year cohort study) 76% decline in diabetes medication use at 12 months post-surgery
Segal: AHRQ 1-Year Cohort Study (2010)76% decline in diabetes medication use at 12 months post-surgery (p≤0.0001) ■ nonsurgical group ◊ surgical group Source: Segal JB, Clark JM, Shore AD, et al. Prompt reduction in use of medications for comorbid conditions after bariatric surgery. Effective Healthcare Research Report No. 28. Rockville, MD: Agency for Healthcare Research and Quality; 2010. (Fig 1, page 14)
Bolen(5 year matched cohort analysis) Lower proportion - and likelihood - of having T2DM at 5 years post bariatric surgery
Bolen: 5-Year Matched Cohort Analysis (2012)Lower proportion – and likelihood - having T2DM at 5yr following bariatric surgery Source: Bolen, Shari and others. Clinical Outcomes after Bariatric Surgery: A Five-Year Matched Cohort Analysis in Seven US States. Obesity Surgery (2012) 22: 749-763, Figure adapted from source data. Non-concurrent, matched cohort study following 22,693 persons who underwent bariatric surgery using logistic regression between groups for up to 5 years.
Swedish Obese Subjects (SOS) Bariatric surgery appears to be markedly more efficient than usual care in the prevention of Type 2 diabetes in obese persons. Carlsson LMS, Peltonen M, Ahlin S et al, Bariatric Surgery and Prevention of Type 2 Diabetes in Swedish Obese Subjects. N Engl J Med 2012; 367:695-704.
Carlsson et al.Significantly lower incidence of Type 2 Diabetes in Bariatric / Metabolic Surgery group at 15 years Carlsson LMS, Peltonen M, Ahlin S et al, Bariatric Surgery and Prevention of Type 2 Diabetes in Swedish Obese Subjects. N Engl J Med 2012; 367:695-704.