Download

1 / 17
190 likes | 328 Views
CLINICAL EFFICACY Oral Telithromycin. George Rochester, PhD, CCRN Statistical Reviewer Division of Biometrics III Division of Anti-infective Drug Products rochesterg@cder.fda.gov. Outline. Phase III clinical database Censored data Clinical or bacteriologic efficacy by indication

E N D
CLINICAL EFFICACYOral Telithromycin George Rochester, PhD, CCRN Statistical Reviewer Division of Biometrics III Division of Anti-infective Drug Products rochesterg@cder.fda.gov
Outline • Phase III clinical database • Censored data • Clinical or bacteriologic efficacy by indication • Overall conclusion
Censored Data • Four investigators were censored by the FDA. • Total number of patients excluded were 186. • Patients were excluded from all indications except T/P. • Both FDA’s and Sponsor’s analyses excluded all subjects from the censored sites.
Phase III Clinical Data • Dosing of interest was for 5 days for AECB, AMS and T/P, and 7-10 days for CAP. • All studies had a designated test-of-cure (TOC) window for assessing the clinical or bacteriologic response. • TOC varied by indication but was always specified in the study protocol.
Definition of Populations • The primary efficacy populations for CAP, AECB and AMS are mITTandPPc. • mITT: All randomized subjects who met disease definition and received at least one dose of study drug. • PPc: mITT subjects minus those with major protocol violations.
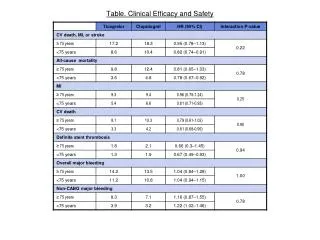
AECB Definitions • Inclusion: Documented history of chronic bronchitis, FEV1/FVC < 70% (tests made in the previous 12 months) • Presentation: cough, sputum volume, sputum purulence, and/or dyspnea • Cure:resolution of all symptoms and no subsequent antimicrobial therapy at TOC
T/P: Regulatory Considerations • Penicillin is the gold standard comparator • Primary efficacy is based on microbiologic eradication • Any product with an absolute eradication rate of < 85% in the PP population should not be considered first line therapy
T/P: Conclusion • T/P is a mild disease • Targeted population is typically children • Many alternative therapies • Insufficient evidence of activity against erythromycin resistant S. pyogenes • Risk/Benefit must be considered
Overall Conclusion • FDA’s efficacy analyses are consistent with those of the applicant. • Adequate, well-controlled trials must demonstrate safety and efficacy.