Download
1 / 25
250 likes | 334 Views
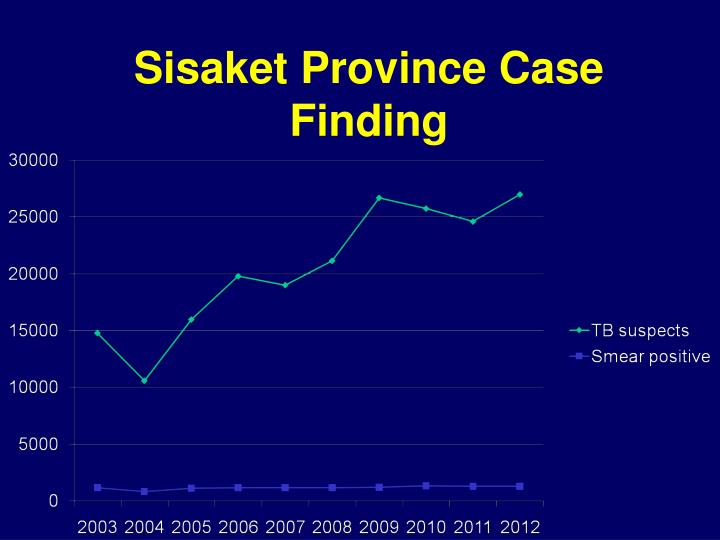
Sisaket Province Case Finding. 2. Recording and Reporting. Quality and completeness of data is impressive Timely submission of reports Initiatives to create own systems to meet program monitoring needs

E N D
2. Recording and Reporting • Quality and completeness of data is impressive • Timely submission of reports • Initiatives to create own systems to meet program monitoring needs • Examples of good integrated systems at local level for both monitoring and case coordination
Recording and Reporting • Multiple paper and electronic data systems: high documentation burden • Specific issues with childhood, MDR TB, TB/HIV data • Examples of good analysis/use of program data at different levels • Some prov/regional data discrepancies
Himpro HOS XP Smart TB TBCM
Recommendations • National level: • Careful review of systems still required to minimize duplication among systems • Assess state of data standards for hospital systems (HIMPro, HosXP, HosOS) to ensure cross-communication • Provincial level: Consider electronic case records to reduce multiple line-list systems
4. TB in Prisons • Longstanding TB screening policy; more systematic approach since 2003 • Strong collaboration in place and clear roles among • Srisaket prison • Srisaket provincial hospital • Srisaket PHO • Challenges of crowding, low staffing
Case Finding • On entry (<1 month): Symptom screening, AFB smear for symptom+ • After entry (>1 month): Periodic awareness raising, diagnostic testing and referral SSK hospital for care-seekers • Very few cases identified from new prisoner screening; most from symptomatic care-seekers
Case Finding (II) • Screening protocol is not sensitive • Symptom questions appropriate • AFB smear (insensitive) • CXR only after SS+ or continued illness on observation in SS- • Good initiative to define populations (new vs. old) for better monitoring
Treatment and Outcomes • SS+ patients are isolated • Coordination with SSK hospital clinical services is strong • Evidence of effectiveness (not fully quantified): sharply decreased death rates • No MDR TB cases to date • Good treatment adherence? • Insufficient testing?
Recommendations • SSK prison: continue monitoring and use of own data; maintain staffing • Dept of Corrections/DDC: review guidance • sensitive screening algorithms, increased use of CXR, including staff • Routine molecular testing for prisoners as MDR risk group • Consider HIV VCT for all given risk groups (review national data)
5. Migrants: Observations • 400-500 registered migrants in SSK; unregistered unknown but likely low • Registered migrants have insurance and access to care • ODPC 7 provides SLDs to 10 people--“marginalized” population who are unable to access NHSO/GPO services
Migrants: Recommendations • Reconsider the definition of vulnerable populations for this province • Prisoners and migrants: where to invest? • Identify strategy for sustainability beyond GFATM for vulnerable populations
6. Laboratory • Microscopy: well resourced, good IQC and EQA system. • Staff skilled and well trained • LED-FM in 2 hospitals, planned for all next year • Both paper and electronic records kept (duplication of work) • Good recording of sputum quality and indication (incl month of f/u)
Laboratory (II) • Sputum containers: aerosol risk • Low slide positivity rate • Sputum quality? • Case finding in low risk population? • Sputum collection booths well designed and located • Good specimen transport systems • BSC class II installed with good maintenance records
Challenges At one hospital: high proportion of sputum specimens are saliva SSK hospital lab not logging specimens sent for culture, DST; incomplete information on ODPC7 request form Monitoring of number of sputum specimens: only done for confirmed cases Two electronic systems not fully integrated: M-lab and HIMPRO
Recommendations Clarify procurement specs for sputum cups (wide mouth, clear, screw cap lid) IQC slide preparation: 1+ slides, not 3+ Review sputum collection patient education: improved sputum quality SSK hosplab: complete info for culture/DST specimens referred Better integration of MLaband HIMpro, or single program
7. MDR TB • 62 cases of MDR-TB in ODPC 7 in 2012 • 6 cases in Sisaket Province • 2 cases in Khuk Khan District • 1 case in Kantaralak District • Culture, DST performed by ODPC 7 • Molecular diagnostics: available in ODPC7 since Jan 2013
MDR TB (II) • Management system works well for 6 patients in Sisaket Province • Provincial hospital manages overall care (treatment regimen, adverse events) • District Hospital oversees DOT, which is done by PCU and VHV
MDR TB (III) • Monthly reporting (Excel) to Sisaket PHO and quarterly case reporting to ODPC7 since this year; NSHO case report • System adequate for current low case load • MDR clinical case reporting to ODPC7 not done until GFATM project (2012) • Lab request/report forms often first notification; not enough patient information for case management
MDR TB: Recommendations • Support clinical management decisions • Monthly (quarterly?) clinical case conferences coordinated by ODPC • Link with BTB MDR-TB network being developed: connecting provincial physicians with national-level experts • Second-line drugs: levofloxacin should replace ofloxacin as soon as possible
Recommendations (II) • Duration of injectables: at least 4 months post conversion • Updated national PMDT guideline in process of finalization • Complex cases should be discussed on case-by-case basis with experts • Diagnostics: NHSO support for follow up cultures, expanded risk categories
8. Childhood TB • TB disease and infection in children is being diagnosed and treated but not necessarily reported to ODPC7 • Low child TB disease prevalence • Child TB 0.2% of the total caseload (10/5224) ODPC7 2012 (national 1.3%) • No TB disease in <5 year olds reported from Sisaket in the last 3-4 years • Child contact management