Download
1 / 43
450 likes | 645 Views
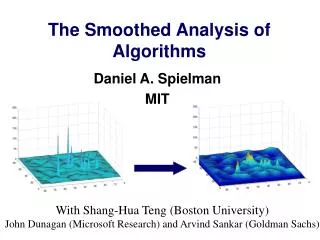
Acyl carnitine analysis: Pitfalls & Problems. Rachel Webster Birmingham Children’s Hospital. Carnitine. Quaternary ammonium compound Biosynthesised from lysine and methionine Liver and kidney Transports fatty acids from cytosol into mitochondria

E N D
Acyl carnitine analysis:Pitfalls & Problems Rachel Webster Birmingham Children’s Hospital
Carnitine Quaternary ammonium compound Biosynthesised from lysine and methionine Liver and kidney Transports fatty acids from cytosol into mitochondria Facilitates the production of energy from fat
Dietary fat Major component of dietary fat is triglycerides 1 glycerol 3 fatty acids
Energy production Preferentially use carbohydrates Glucose Glycogen Hypoglycaemia (fasting, illness, infection) Fat metabolism Mitochondrial oxidation of fatty acids provides upto 80% of total requirement Protein metabolism Last resort Periods of excessive starvation
Transport into mitochondria Acyl-CoA Carnitine Transporter
Acyl co-A dehydrogenase species SCAD C4-C6 MCAD C4-C12 LCAD C8-C20 VLCAD C12-C24
Energy yield Fat 106 ATP 1 molecule of C16 palmitate Carbohydrate 36 ATP 1 molecule of glucose Why we only need a small amount of fat in our diets
Defects Carnitine deficiency CPT-1 deficiency CPT-2 deficiency CACT (carnitine transporter defect) VLCADD LCADD MCADD SCADD Plus many more!!! all differing acyl carnitine profiles
Free and acyl carnitine analysis Native (underivatised) acyl carnitines Butylated derivatives Carboxylic acid group is esterified Both fragment to yield a common m/z 85 daughter ion
BCH Practice Paired DBS and plasma CIL NSK-B IS kit Derivatise Report Quantitative free carnitine (plasma) Qualitative acyl carnitine interpretation (plasma & DBS) Quantitate any relevant species Underivatised Urgent samples Unusual peaks
BCH Practice DBS and Plasma Plasma Acute scenario DBS Better overview of long-term status Some disorders are better represented in different sample types GA-1 HMG CoA Lyase deficiency
Sample preparation Derivatised Underivatised 3mm DBS 10ul plasma 200ul IS c stable isotopes 30min elution Dry Protein crash Butanol HCL Dry Direct flow injection +ve ESI MSMS
BCH Practice • Acyl carnitines • Parents m/z 85 scan • Currently generating age-related reference ranges • Free carnitine quantitation • MRM 218 > 85 • Ref range 13-53 umol/L • Linearity 300 umol/L • Chromsystems Neonatal Screening IQC • CDC EQA DBS Scheme • ERNDIM Free carnitine Scheme
Internal Standard - Deriv C0d9 C2d3 C16d3 C5d9 C14d9 C4d3 C3d3 C8d3
Advantages of derivatisation Increased mass compared to underivitised avoids low mass contaminants solvent adducts Less affected by ‘isobaric conflicts’ dicarboxylic acylcarnitines C3DC hydroxycarboxylic acylcarnitines [OH]C4 Better ionisation of dicarboxylics 2 COOH gps Double derivitisation Increased positivity excellent for +ve ESI Culture established worldwide published data better understanding of analysis
Underiv - ?Malonyl/OHBut Patient 1 m/z 248 Patient 2
Deriv - ? Malonyl/OHBut m/z 360 ie malonyl carnitine C3DC Patient 1 m/z 304 ie hydroxy butyryl carnitine Patient 2
Disadvantages to derivatisation For big batches (screening)…time, effort, cost and acid corrosion……!!! More steps to method - potential for more errors Hydrolysis during derivatisation loss of acylcarnitines increase in free carnitine Isobaric conflict Acetylcarnitine and glutamate m/z 260…esp DBS dicarboxylic acylcarnitines and hydroxyacylcarnitines [OH]C8 [OH]C10 ‘pseudo-glutaryl carnitinaemia’ in MCADD
SCADD Diagnostic peak m/z 288
MCADD - crisis Diagnostic peak m/z 344
VLCADD Diagnostic peak m/z 426
Ketotic Peaks m/z 260, 304 & 426
GA1 DBS vs Plasma - Deriv Diagnostic peak m/z 388
GA1 Plasma Deriv vs Underiv Diagnostic peak m/z 388 Diagnostic peak m/z 275
GA2 Diagnostic C4 – C18
b ketothiolase deficiency Diagnostic peaks m/z 300 & 318
MMA Diagnostic peaks m/z 274 & 374
PA Diagnostic peak m/z 274
IVA Diagnostic peak m/z 302
Malonic aciduria Diagnostic peak m/z 360
PMB Increased free and short chains
Acylcarnitine MRM (butyl) MRM (underiv.] Disorder C0 218 > 85 162 > 85 PCD C2260 > 85 204 > 85 (Glutamate) C3 274 > 85 218 > 85 MMA; PA C4 288 > 85 232 > 85 EMA;SCAD; GA2 C5:1 300 > 85 244 > 85 PA; BkT C5 302 > 85 246 > 85 IVA; GA2 C4-OH304 > 85248 > 85 (Ketosis) C6 316 > 85 260 > 85 GA2 (MCAD) C5-OH318 > 85262 > 85 Biot;IVA;BkT;3HMG C8344 > 85288 > 85MCAD / [?] C3-DC360 > 85248 > 85 Malonic Aciduria C8-OH360 > 85304 > 85 (Metab Crisis) C10:1 370 > 85 314 > 85 MCAD C10 372 > 85 316 > 85 GA2 C4-DC374 > 85262 > 85 [MMA] C5-DC388 > 85276 > 85 GA1 ; (GA2) C10-OH388 > 85332 > 85 (Metab crisis) C12:1 398 > 85 342 > 85 [B-oxidn] C12 400 > 85 344 > 85 (B-oxidn]
Plasticisers Diagnostic peak m/z 288
Additional peaks Benzoate m/z 332 Phenylbutyrate m/z 336 Cefotaxime m/z 470 & 426
Cefotaxime Two peaks m/z 426 & 470
Conclusions Isobaric compounds Deriv vs underiv Which ever method run routinely must be ready to run other way for confirmation Plasma vs DBS Plasticisers