Download
1 / 71
810 likes | 930 Views
Hypersensitivity. Láng, Orsolya MD, PhD Dept. Genetics, Cell & Immunobiology, Semmelweis University. www.dgci.sote.hu. Lecture ED 2015. Hypersensitivity - Tolerance. Hypersensitivity:

E N D
Hypersensitivity Láng, Orsolya MD, PhD Dept. Genetics, Cell & Immunobiology, Semmelweis University www.dgci.sote.hu Lecture ED 2015
Hypersensitivity - Tolerance Hypersensitivity: Immune reaction leads to pathology upon recognition of either harmless environmental antigens or self-antigens Tolerance: immunological unresponsiveness to (self)-antigens (tolerogen) that have the capacity to elicit an immune response Autoimmunity: Autoreactivity is inevitable Dysregulation or failure of self-tolerance => autoimmune disorder Common: adaptive immune system
Hypersensitivity (HS) – Allergy • The most common immunological abnormality. • Increasing number of affected people (25-40%) • Potential reasons: Environmental pollution (?) • Lack of selection (?)
General mechanism First exposure Repeat exposure Tissue injury or disease Sensitization • Robert Royston Amos ("Robin") Coombs: • British immunologist, • co-discoverer of the Coombs test (Arthur Mourant and Rob Race) in 1945 Gell - Coombs classification of hypersensitivity in 1963
Four classifications • Type I (Immediate) hypersensitivity • Type II (cytotoxic) hypersensitivity • Type III (immune complex mediated) hypersensitivity • Type IV (delayed) hypersensitivity
Type I. hypersensitivity (HS) Immediate HS or Allergy , Atopy Atopy – inherited tendency to respond immunologically to inhaled or ingested allergens with increased IgE production
Commontypes of immediate HS Skin contact Inhaled allergens Ingestion Hives Urticaria Food allergies Hay fever or injection Bronchial asthma Anaphylaxis
Main characteristics of the allergenes • Smallsizeproteinsorglycoproteins: • Carried on desiccated particles (pollen grains or mite feces), where they are very stable • Haveenzymeactivitythatfacilitatethetransmucosalpenetrance • Small, molecularwheight is 5 to 70 kDa (dustmite: der p1 15 kD), • Highsolubility • Smalldose(ragweed: 1µg/year) • MHCII binding
What do they have in common? ? Hevein domain
Cross-reactive allergenes http://ainotes.wikispaces.com/Pollen+Food+Allergy+Syndrome
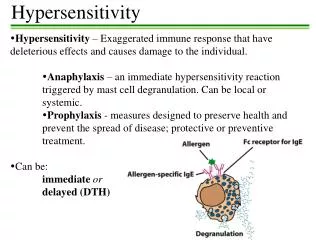
Type I. hypersensitivity Afferent phase Hypersensitivity IgEproduction IL4, IL13 Degranulation Firstexposure APC and Th2 activation Classswitch IgEproduction IgE+ memoryB-cells cross-linkedIgE Mastcells Basophils FcᵋRI receptor Repeatexposure ACTIVATION and DEGRANULATION Nature Review, Drug Discoverys alapján
Classswitch of BCR genes INF IL5 IL-4 IL-13
Fcereceptors onmastcellsand basophils FcƐRI(highaffinity) Kd= 10-11 M [IgE] = 10-9 M MC arealwayscoatedwith IgEboundreceptors FcƐRIIa on B cells FcƐRII(lowaffinity) FcƐRIIb (CD23) on B cells, T cells, Mφ-s, DC-s and basophils
Effects of IgE cross-linking (phospholipids)
Degranulation of MC • Other degranulators • Immune • Anaphylatoxins: C5a, C3a • Modulator • IL3 • Non Immune • Bacterial products, gastrine, physical (cold), stress, chemical (gases, smoke), etc. • Intracellular signalling: Ca++ • Inhibitors of degranulation • Pharmacotherpy: cromoglicinum
Pro-inflammatory mediators released by mast cells, basophils and eosinophils Primary mediators are in preformed granules Gilfillan et al.Nature Reviews Immunology 6, 218-230 (March 2006) | doi:10.1038/nri1782
Histamineis thekeymediator and theirreceptors H1: e.g GIT, bronchoconstriction↑; vesselpermeabilty↑ H2: e.g. vasodilataion ↑; secretion of exocrinegland(e.g. gastricacid)↑; secretion (H3: neuralsystem) H4: eosinophilchemotaxis
Role of the Mast cells (MC) MC (Connectivetissue) MucosalMCs Intravenous , high dose Subcutanous, low dose Ingestion Inhalation, low dose capillaries capillaries SM in brochus SM in intestin Systemic anaphylaxis urticaria Hay fever, Bronchial asthma Food allergy: diarrhea, vomiting utricaria, anaphylaxis
Immediate reaction in respiratory tract Nature Medicine 18, 693–704 (2012) doi:10.1038/nm.2755
Immediate and late phase symptoms PEFR = peak expiratory flow rate After 2 hrs After 1 day
Chronic inflammation and complications (tissue remodelling) Nature Medicine 18, 693–704 (2012) doi:10.1038/nm.2755
Atopy • Atopy is the term for the genetic trait to have a predisposition for localized anaphylaxis. • Atopic individuals have higher levels of IgE and eosinophils.
Allergy – Multifactorial disorder Genetics FcƐRI beta chain - 11q13 IL-3, IL-4, IL5, IL-9, IL-13 and GMCSF coding genes - 5q31 MHCII allels - 6p Allergy Environmental factors Failure of tolerance during childhood Dysregulaion of the Immune system Activation of Th1 and Th2 subpopulation IgE production Immunodeficiency Increased eosinophil count
DER p1 in the faeces of the house dust mite penetrates the airway epithelium
Bronchialasthma normalbronchiole severe asthma
Anaphylaxis • Anaphylactic shock is the most serious • Symptoms are directly related to the massive release of vasoactive substances leading to fall in blood pressure, shock, difficulty in breathing and even death. • It can be due to the following: • Horse gamma globulin given to patients who are sensitized to horse protein. • Injection of a drug that is capable of acting as a hapten into a patient who is sensitive, ie, penicillin. • Following a wasp or bee sting in highly sensitive individuals. • Foods – peanuts, shellfish, etc.
StaphylococcusexotoxinsmayserveeitherassuperantigensorallergensStaphylococcusexotoxinsmayserveeitherassuperantigensorallergens Non specific T-cell activation !
Therapy • Avoidance of known allergens • Localized reactions use OTC antihistamines and decongestants. • Asthma uses combination – antihistamines, bronchodilators and corticosteroids. • Systemic use epinephrine • Hyposensitization – inject antigen to cause production of IgG which binds to antigen (allergen) before it reaches IgE coated cells. • Monocolonal anti-IgE– inject, binds to receptors on mast cells blocking them from the IgE.
Administration of increasing doses of antigen desensitization
DESENSITIZATION – Allergen-specific immunotherapy Repeated administration of the sensitizing allergen usually by subcutaneous injection or, more recently, by sublingual application. Both IgE- and IgG-specific antibodies increase during postdesensitization therapy. IgGactsasblocking Ab http://www.fpnotebook.com http://www.voedselallergie.nl/allergic-and-non-allergic-hypersensitivity-to-food
Anti-IgE therapy Monoclonal antibody Nature Reviews Immunology 8, 218-230 (March 2008)
In vivo test - Intradermalallergy test (Pricktest) • Small amount of allergen injected into skin • Look for wheal formation of 3mm or greater in diameter • Simple, inexpensive, can screen for multiple allergens. • Stop anti-histamines 24-72 hours before test. • Danger of systemic reaction • Not for children under 3
In vitro test • Measure total IgE or antigen-specific IgE in serum • Less sensitive than skin tests. • RIST, RAST, Allergen specific and Microarray will be covered later. Protein array RAST RadioAllergoSorbent Test
Anaphylaxis vs. Anaphylactoidreaction (pseudoallergy) Ibuprofen v. COX1 inhibitor No test! 4 type of pseudoallergybasedon COX1 inhibition http://allergycases.blogspot.hu/2010/07/allergic-and-pseudoallergic-reactions.html
Type II. hypersensitivity Cell surface antigen (IgG v. IgM) Antigens: Intrinsic - autoantigen, Membrane component(receptor) Extrinsic antigen RBC – tarnsfusion, Rh incompatibility Absorbed drugs or metabolits
Pathomechanisms of type II. hypersensitivity Opsonization => phagocytozis Fc-receptor mediated phagocytosis/ cell lysis (macrophage, NK cell, neutrophil & eozinophil) Complement activation=> cell lysis ADCC (antibody dependent cellular cytotoxicity) Abnormal physiologic response: Ab inhibits binding of neurotransmitter anti Ach R: myasthenia gravis Ab stimulate receptor anti-TSH R: autoimmune thyroiditis
Hemolysis Transfusion reaction Incompatible transfusion - IgM Polytransfused - IgG Multipara - IgG Rh incompatibility Complication: Erythroblastosis fetalis Not only RBC, but Platelets or leukocytes
Erythroblastosis fetalis Haemolytical disease of the newborn
Erythroblastosis fetalis Passive immunization with anti-Rh
Haemolytic anaemia and thrombocytopeny Drugs/ metabolits can act as a hapten – e.g. penicillin
Autoimmune thyroiditis Graves- Basedow + exophtalmus Altering signal transduction Myastenia Gravis - ptosis 3 hrsaftermethylprednisolontreatment
Type III. HS Soluble antigen-antibody complex - IMMUNE COMPLEX disease
Pathomechanism Solubile Ag - Ab (IgG or IgM) => IC => Complement activation=> inflammation and tissue injury Mechanism of the tissue destruction similar in all tissue Severity depends upon: size of the IC, ratio of Ag/Ab, affinity of Ab, isotype of Ab
The consequence of the tissue damage depends on the site of deposition 1. Local immune complex disease Arthus reaction – skin necrotic vasculitis – vascular wall pneumonitis – farmer’s lung 2. Acute-systemic immune complex disease acute serum disease (7-10 days) 3. Chronic immune complex disease SLE Rheumatoid arthritis