Download
1 / 18
190 likes | 412 Views
Treatment of Acute Coronary Syndrome with ST elevation ESC guidelines 2008. Dr. David Tran A&E dept. FVH 22/12/09. Initial diagnosis & early stratification . Chest pain or discomfort First ECG showing persistent ST elevation Elevated biomarkers of necrosis (2D echocardiography).

E N D
Treatment of Acute Coronary Syndrome with ST elevationESC guidelines 2008 Dr. David Tran A&E dept. FVH 22/12/09
Initial diagnosis & early stratification • Chest pain or discomfort • First ECG showing persistent ST elevation • Elevated biomarkers of necrosis • (2D echocardiography)
Relief pain & anxiety • Morphine 0.1mg/Kg loading dose followed by 2mg bolus • Oxygen if breathless or desaturation
Reperfusion strategies • PCI = invasive reperfusion • Fibrinolysis = pharmacological reperfusion
Primary PCI strategy • Time between first medical care & balloon < 90 min • Medical treatment: Aspirin, Clopidogrel and Heparin
Primary fibrinolytic strategy • If PCI cannot be performed within 90 min. • In the absence of contraindications • Associated treatment: Aspirin, Plavix & Heparin
Problems of bleeding complications after fibrinolyse • Intracranial bleeding = 1% • Major non cerebral bleeding = 4-13%
Facilitated PCI ? • No place for a prior fibrinolytic treatment before a planned PCI…
Anti-platelet co-therapies • Aspirin 250mg • Plavix 600mg (PCI) or 300mg (fibrinolytic)
Antithrombin co-therapies • Unfractionated heparin iv bolus 100 UI/Kg • Enoxaparin iv bolus 30mg followed by s.c. dose of 1mg/Kg/12h
Therapy without reperfusion strategy or view later (>12h) • Aspirin • Plavix • Anti-thrombin agent (heparin or Enoxaparin)
Management of arrhythmias in acute phase of ACS • Cardioversion • Amiodarone • Beta blocker
Problem of betablockers • Early use of iv beta-blockers has to be conterbalanced by the risk of cardiogenic shock
Problems of nitrates • The routine use of nitrates in the initial phase of a STEMI is not recommended
Interest of Statins in the acute phase of STMI • MIRACL study: 80mg Atorvastatin in the first days of an acute coronary syndrome > 26% less of recurrent ischemia • PROV-IT study: 80mg Atorvastatin versus 40mg Pravastatin > 29% less of recurrent instable angina with 80mg Atorvastatin • A to Z study: 40mg Simvastatin versus placebo > less cardiovascular mortality
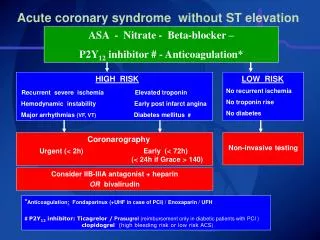
Acute Coronary Syndrome (ACS) • ECG 12 derivations • +/- V7,V8, V9, V3r, V4r • Troponine (if pain > 6h) ACS with ST elevation ACS without ST elevation • First medical treatment • ASPEGIC 250mg IV • PLAVIX300mg loading dose (4tab. 75mg) • LOVENOX 0.1ml/10Kg of weight s/cut. • LIPITOR 80mg high dose (4tab. 20mg) • Metoprolol 50mg if pulse > 80/min, TA >120 • ISOKET IV if persistent chest pain (TA > 120) • Morphine bolus IV If severe pain • First medical treatment • ASPEGIC 250mg IV • PLAVIX 600mg loading dose (8 tab. 75mg) • Heparine70UI/Kg IV loading dose • Morphine 0.05mg/Kg IV first dose • Atorvastatine 80mg • Improvement? • Chest pain relieved or decreased • Patient stable (pulse, pressure) • Next ECG stable or improved • Primary PCI reperfusion • Contact Tam Duc Hospital for agreement • Transfert the patient with SMUR • Ideal timing < 45 min. between 1st ECG and arrival in cathlab. NO YES • Hospitalazation in USC/ICU • Agreement of cardiologist • Refer to cardiologist Transfert to an Hospital with cathlab & cardiologic intensive care