Download

1 / 25
290 likes | 766 Views
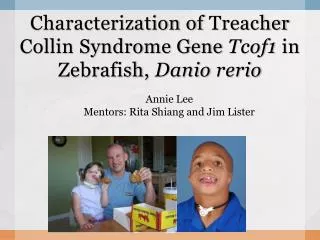
Treacher Collins syndrome. By R2 黃信豪. History (1). This 4 y/o female is a victim of Treacher-Collins syndrome. Multiple facial anormaly including hypoplastic ears, anti-Mongoiian eyes, mandibular facial dysosteosis , micrognathia, and choanal atresia were noted at birth. History (2).

E N D
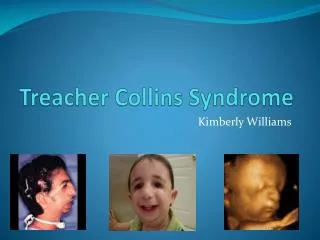
Treacher Collins syndrome By R2黃信豪
History (1) • This 4 y/o female is a victim of Treacher-Collins syndrome. • Multiple facial anormaly including hypoplastic ears, anti-Mongoiian eyes, mandibular facial dysosteosis , micrognathia, and choanal atresia were noted at birth.
History (2) • Due to dyspnea and poor feeding, the p’t was send to pediatric department of NTUH. • Endo-trachea tube intubated for pneumonia was done at that time. • Because of extubation difficulty, tracheostomy was performed on 87-11-28.
History (3) • Distraction of mandible has performed twice on 91-4-26 and 91-11-29. • This time, for the purpose of remove tracheostomy, choanal plasty and stenting were arranged on92-4-15.
History (4) • Past history: • Treacher-Collins syndrome with a. micrognathia s/p distraction twice. b. bil. microtia with hearing aid. c. PFO and PDA d. bil. Choanal atresia s/p tracheostomy. 2. Family history: denied.
What is treacher-Collins syndrome?(1) • It is a condition in which the cheek bones and jawbone are underdeveloped. • Dr. Treacher Collins, a British ophthalmologist, was the first one who described the syndrome in 1900.
What is treacher-Collins syndrome?(2) • Franceschetti and Klein, who extensive reviewed the essential components of the condition, used the term mandibulofacial dysostosis to describe the clinical features. • Treacher Collins-Franceschetti syndrome 1 (TCOF1) was the other named of the syndrome.
Why and how does Treacher-Collins syndrome happen? (1) • There are two possible ways that the syndrome develops: 1. Develop as a new mutation. 2. Inheriting it from one of the parents. • The incidence of the syndrome is about 1 : 10000~1 : 50000
Why and how does Treacher-Collins syndrome happen?(2) • The syndrome is an autosomal dominant disorder. • The gene mutated in this syndrome was mapped at 5q32-33 initially. • Two apparently balanced translocations, t(6;16)(p21.31;p13.11) and t(5;13)(q11;p11), and two interstitial deletions, del(4)(p15.32;p14) and del (3)(p23;p24.12)
Clinical features and diagnosis of the syndrome (1) The anomalies was due to the defects of the first and second branchial arches, clefts, and pouches during early embryonic development : • Abnormalities of the pinnae which are frequently associated with atresia of the external auditory canals and anomalies of the middle ear ossicles. Bil. Conductive hearing loss is common.
Clinical features and diagnosis of the syndrome (2) 2. Hypoplasia of the facial bones, especially mandible and zygomatic complex. • Antimongoloid slanting of the palpebral fissures with colobomata of the lower eyelids and a paucity of lid lashes medial to the defect. • Cleft palate .
Clinical features and diagnosis of the syndrome(3) • The clinic features are usually bilaterally symmetrical, and the non-penetrance is rare. • But due to the expression of the gene is extremely variable, the diagnosis and subsequent genetic counselling may be very difficult.
Clinical features and diagnosis of the syndrome(4) • The minimal diagnostic criteria for the syndrome: a. 40% of cases have a previous family history. b. cranio-facial radiographs, particularly the occipito-mental view. c. chromosome and gene exam.
What problems can be expected?(1) • The most common difficulties involve: a. breathing b. hearing c. vision
What problems can be expected?(2) • The reasons that may cause breathing problems: • Small or undeveloped jaw • Cleft palate and choanal atresia • Tongue drop • Pharyngeal hypoplasia
What problems can be expected?(3) • Dyspnea while developping colds and infections due to congestion and swelling of the airway. • Sleep apnea – affect the child’s mental development. • Speech therapy was needed.
How to establish a safe airway? • There some methods to help to establish a safe airway : 1. intubation with laryngoscope 2. tracheostomy 3. use augustine stylet 4. translaryngeal guided intubation
The role of a anestheiologist • This doctor is a very important part of any craniofacial team. Children with craniofacial problems often have problems associated with the airways that create breathing difficulties. It is essential that this doctor be well trained in pediatric anesthesiology, but it is just as important that he/she have substantial experience in dealing with these special children. The pediatric anesthesiologist’s amount of experience with craniofacial problems perhaps has the greatest effect on the overall safety of the surgery.