Download
1 / 0
0 likes | 150 Views
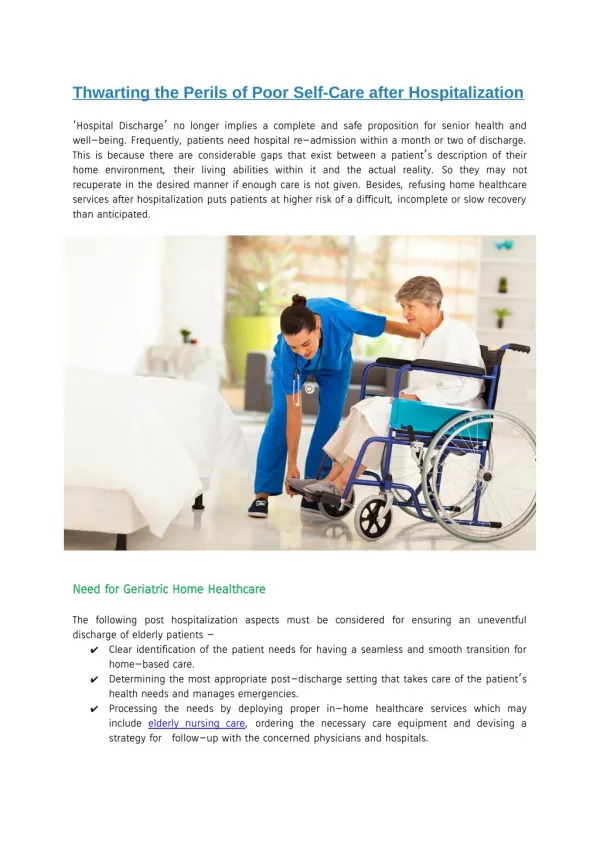
Medicine, Disease and Society in Britain, 1750 - 1950. Medicine, Charity and the Care of the Poor. Lecture 4. Lecture Themes. Links between sickness and poverty Access to medical care for the poor Increasing population, urbanisation and industrialisation Increasing pauperism

E N D