Download
1 / 23
230 likes | 236 Views
GUSTO-IV Pilot Trial. SPEED. Rationale for Combination Therapy in AMI. Enhance Incidence and Speed of Reperfusion Reduced Mortality Safer Therapy - Less IC bleed Facilitate Early Percutaneous Interventions. ACC 1999: Oral Presentation. SPEED. Rationale for Combination Therapy in AMI.

E N D
SPEED Rationale for Combination Therapy in AMI • Enhance Incidence and Speed of Reperfusion • Reduced Mortality • Safer Therapy - Less IC bleed • Facilitate Early Percutaneous Interventions ACC 1999: Oral Presentation
SPEED Rationale for Combination Therapy in AMI • Improved Reperfusion • Only 40-50% achieve normal perfusion (TIMI grade 3 flow) with fibrinolytic therapy alone • Reduced Mortality • 30% 1-year mortality among the elderly (> 75 years)in GUSTO-III ACC 1999: Oral Presentation
SPEED Rationale for Combination Therapy in AMI • Reduced ICH Rates • 21% increase in IC bleed from GUSTO-I to GUSTO-III with t-PA • Facilitate Early Percutaneous Interventions • Improved mortality with primary PCI is limited tohospitals where procedure and expertise is available ACC 1999: Oral Presentation
SPEED Overview of Trials of Low-Dose Lysis and GP IIb/IIIa Inhibitors TIMI -14 SPEED/GUSTO IV AMI Pilot Criteria Age 18 to 75 Symptoms < 12 hours > 18 years old Symptoms < 6 hours Control Arm(s) Accelerated t-PA and 10 U +10 U Reteplase Standard Reteplase 10 U +10 U Combination Therapies Studied t-PA, SK, or Reteplase + Reteplase + Abciximab* with Abciximab* with Heparin 60 U/kg 30 U/kg Heparin 60 U/kg 40 U/kg 1° Endpoint TIMI grade 3 flow at 90 minutes TIMI grade 3 flow at 60-90 minutes (avg. was 62 min) PCI “Encouraged” -Facilitated PCI Rescue only * bolus 0.25 mg/kg; infusion 0.125mg/kg/min x 12h ACC 1999: Oral Presentation
SPEED Ability of Abciximab to Cause Dethrombosis TIMI Grade 3 flow Study Time 25% 0 50% Gold et al 10 min Circ. 1997; 95: 1755-59 GRAPE 45 min JACC 1999; 33:1528-32 SPEED 60 min EHJ 1999; 20:616 (#3336) TIMI-14 90 min Circ. 1999; 99:2720-32 8% 18% 23% 32%
1:1 Randomization r-PA 10 + 10 U Heparin 70 U/kg Abciximab standard dose r-PA 5 + 5 U Heparin 60 U/kg / 40 U/kg 60-90 Minute Angiography PTCA + Stent as indicated SPEED Dose Confirmation Protocol • Acute MI • ST elevation • Symptom duration < 6 hrs. Administered in the ED ACC 1999: Oral Presentation
SPEED Dose Escalation and Confirmation Experimental Abciximab Abciximab + r-PA + r-PA 5 U + 5 U n = 166 60 U heparin n = 76 Control Abciximab Alone n = 63 Dose Escalation Experimental Abciximab Abciximab + r-PA 5 U + 5 U + r-PA 5 U + 5 U 60 U Heparin 40 U Heparin n = 40 n = 76 Control r-PA 10 U + 10 U n = 109 Dose Confirmation Total Abciximab + r-PA 5 U+ 5 U + 60U Heparin, n=116 ACC 1999; Oral Presentation
Dose ConfirmationAcute Cardiac Catheterization Abciximab r-PA 5 + 5 60 U Hep (n = 40) Abciximab r-PA 5 + 5 40 U Hep (n = 76) r-PA Alone (n = 109) Time from study 60 (50,65) 55 (48,61) 60 (48,67) drug to cath (min)* Infarct-related artery: LAD 41% 32% 45% LCX 14% 16% 9% RCA 44% 49% 45% PCI of IRA 83% 70% 94% at 60-90 min * median (25th, 75th) ACC 1999: Oral Presentation
SPEED TIMI Grade 3 Flow at 60-90 Min Angiographic Core Lab Reading by Treatment Recieved p = 0.395 n = 107 n = 34 n = 75 n = 109 r-PA Alone 60 U Hep Abciximab + r-PA 5 + 5 40 U Hep Abciximab + r-PA 5 + 5 Total ACC 1999: Oral Presentation
SPEED TIMI Grade 3 Flow at 60-90 Min Angiographic Core Lab Reading p = 0.06 p = 0.2 n = 107 n = 103 n = 75 n = 66 r-PA Alone 60 U Hep Abciximab + r-PA 5 + 5 40 U Hep Abciximab + r-PA 5 + 5 Abciximab Alone ACC 1999: Oral Presentation
SPEED Median TIMI Frame Count by Treatment Received Dose escalation and confirmation 100 p = 0.87 p = 0.43 43 36 33 60 U Hep Abciximab + r-PA 5 + 5 40 U Hep Abciximab + r-PA 5 + 5 Abciximab Alone r-PA Alone ACC 1999 : Oral Presentation
SPEED Clinical Outcomes* Abciximab r-PA 5 + 5 60 U Hep Abciximab r-PA 5 + 5 40 U Hep r-PA Alone Abciximab Alone Death 5.6% 4.4% 2.6% 3.2% Reinfarction 2.8% 1.7% 1.3% 0% Severe ischemia 2.8% 4.3% 2.6% 6.4% requiring urgent revascularization Composite 11.2% 9.6% 5.3% 9.5% * to 30 days post randomization ACC 1999: Oral Presentation
SPEED Rationale for Facilitated PCI • Meta-analyses suggest improved survival withprimary PTCA over lysis • Procedural success lower in vessels with TIMIGrade 0-1 vs. 2-3 • Limitations to primary PTCA include access(minority of hospitals can perform PCI) and delayin restoring flow (few hospitals < 60 min to cath) ACC 1999: Oral Presentation
SPEED Facilitated PCI 530 Patients 464 Patients 60-90 min cath TIMI Grade 0-1 (n = 136) TIMI Grade 2-3 (n = 324) 323 Patients PCI PCI 91% No PCI 9% PCI 61% No PCI 39% ACC 1999: Oral Presentation
SPEED Facilitated PCI Procedural Outcome Pre-Procedure TIMI Grade Flow 0-1 (n = 123) 2-3 (n = 198) Post-Procedure p Final diameter stenosis 10 (0, 25) 0 (0, 20) 0.0001 TIMI grade 3 flow 83% 95% 0.001 Stents 73% 81% 0.09 Procedural success* 81% 93% 0.001 * < 50% diameter stenosis with TIMI grade 3 flow ACC 1999: Oral Presentation
SPEED Facilitated PCI Clinical Outcome TIMI Grade Flow 0-1 (n = 123) 2-3 (n = 198) Death 4.1% 3.0% Reinfarction 2.4% 0.5% Severe ischemia 1.6% 1.5% requiring repeat revascularization Composite 7.3% 4.6% Blood transfusion 7.3% 10.1% ACC 1999: Oral Presentation
SPEED Facilitated PCI TIMI GRADE 2-3 Flow Early (60-90 min) PCI Late* PCI Abciximab alone 52% 83% 3% (n = 66) Abciximab + r-PA 5 + 5 76% 66% 11% (n = 192) r-PA alone 73% 61% 10% (n = 109) * > 24 hours after randomization ACC 1999: Oral Presentation
SPEED Facilitated PCI Procedural Outcome Abciximab Alone (n = 40) Abciximab + r-PA 5 + 5 (n = 114) r-PA Alone (n = 60) Post-Procedure p** Final diameter stenosis 10 (0, 25) 5 (0, 25) 5(0, 20) 0.41 TIMI grade 3 flow 95% 90% 85% 0.16 Stents 75% 75% 90% 0.02 Procedural success* 95% 88% 85% 0.35 * < 50% diameter stenosis with TIMI grade 3 flow ** compares any abciximab to r-PA alone ACC 1999: Oral Presentation
SPEED Facilitated PCI Clinical Outcomes Abciximab Alone (n = 40) Abciximab + r-PA 5 + 5 (n = 114) r-PA Alone (n = 60) Death 5.0% 5.3% 3.3% Reinfarction 0% 1.8% 1.7% Severe ischemia 5.0% 0.9% 1.7% requiring repeat revascularization Composite 10.0% 6.1% 6.7% Blood transfusion 5.0% 9.7% 6.7% ACC 1999: Oral Presentation
Conclusion • Low dose fibrinolytic therapy in addition to abciximab improves reperfusion rates • Heparin dose with the combination is also important to maximize reperfusion rates with abciximab + low-dose r-PA • Combination therapy appears to facilitateearly PCI in AMI
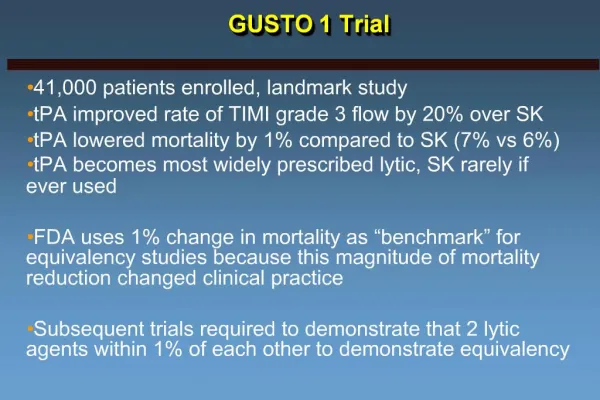
Results in a Perspective GUSTO-1 90-min Meta-analysis 60-min SPEED 60-min 100% p < 0.001 p = 0.06 14% 23% 23% 75% 54% 50% 31% 25% 0% Abciximab r-PA 5 + 5 SK t-PA ACC 1999: Oral Presentation
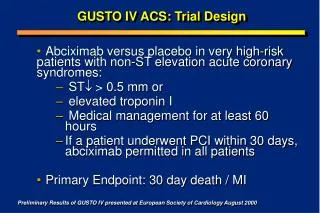
GUSTO-IV AMI Trial Protocol (n = 16,600) ST , lytic eligible, < 6 h ASA No Abciximab Abciximab* 2 x 10 U bolus (30’) Reteplase 2 x 5 U bolus (30’) Reteplase Standard Heparin: 5,000 U bolus followed by either 800 U/hr (pts < 80 kg) or 1,000 U/hr (pts > 80 kg) infusion Low Dose Heparin: 60 U/kg bolus followed by a 7 U/kg/h infusion 1º endpoint: mortality at 30 days 2º endpoint: clinical and safety events at 30 days * 0.25mg/kg bolus followed by 0.125 g/kg/min infusion for 12 hours