Download

1 / 45
450 likes | 646 Views
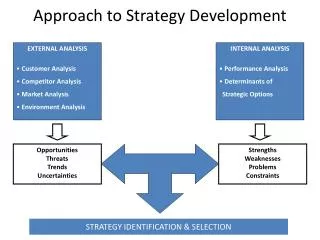
The NCI Approach To Drug Development. Edward A. Sausville, M.D., Ph.D. Developmental Therapeutics Program National Cancer Institute. Goals Of Preclinical Drug Studies. Scientific framework. Discovery of “lead structures”

E N D
The NCI Approach To Drug Development Edward A. Sausville, M.D., Ph.D. Developmental Therapeutics Program National Cancer Institute
Goals Of Preclinical Drug Studies Scientific framework • Discovery of “lead structures” • “Refinement”: chemistry, pharmacology, efficacy =“Early” development • Late development: formulation, dose form, toxicology
Goals Of Preclinical Drug Studies Regulatory framework • IND = “Investigational New Drug” application • = approval by FDA to conduct human studies; • main criterion : SAFETY AND LIKELY REVERSIBLE TOXICITY = allows start of Phase I trials • NDA = “New Drug Application” • = basis for sale to public; • main criteria: SAFETY AND SOME MEASURE OF EFFICACY = result of Phase II/III trials
Treatment A % Alive Treatment B or no R x Time R x Untreated R Cytostatic x Tumor Size Time Cancer Drugs:How Do We Know We Have A Winner? - PHASE III CLINICAL TRIAL = WINNER - PHASE II = POTENTIAL WINNER ; Time? - PRECLINICAL MODEL (e.g., mouse or rat) Cytotoxic
Cancer Drugs: How To Pick A Winner? “VALIDATED” CANCER TARGETS • DNA • Alkylators • Antimetabolites • Topo I / II • Tubulin • Receptors • Nuclear • Cell Surface (Immune?) • Oncogene Proteins (2001: AT LAST!)
SCREEN PHARMACOLOGY + ANTI-TUMOR ACTIVITY!! (in vitro/in vivo) CHEMISTRY OPTIMIZED SCHEDULE (in vivo) IND-DIRECTED TOX/FORMULATION PHASE I: DOSE/SCHEDULE HUMAN PHARM/TOX PHASE II: ACTIVITY = SHRINKAGE PHASE III: COMPARE WITH STANDARD “Empirical” Drug Discovery
Problems With Empirical Models • Lack of predictive power in vivo • Poor correlation of non-human with human pharmacology • Divorced from biology • Inefficient: many compounds screened; • developed, but have “late” = clinical trials outcome • at Phase III to define “validation” of compound action
Deacylation SAN-Gly H3C(CH2)8CH=CHCH=CHCO2H Protein Synthesis KRN5500 Cell Membrane
vehicle 13.5 qdx5 33.5 q4dx3 22.4 q4dx3 20 qdx5 50 q4dx3 30 qdx5 5000 4500 4000 3500 3000 2500 2000 1500 1000 500 0 + X Median Tumor Weight (mg) 8 12 15 18 22 26 29 33 36 41 Day Posttumor Implantation Effect Of KRN5500 On Colo-205 Athymic Mouse Xenografts
KRN5500 Plasma Concentrations On Effective Schedule(20 mg/kg/d) In Mice Plasma Concentration (M) Time (days)
Summary Of KRN5500 Phase I • 26 patients as IV once per day over 5 days • Dose limiting toxicity = interstitial pneumonitis • MTD = 2.9 mg/M2/d x 5 • Achieve only 0.75 - 1 M at 3.7 mg/M2/d x 5 • 4/6 patients with >25% incr Cmax have grade 4 toxicity Data of J. P. Eder, DFCI
In Vivo i.e., Intact Animal Tumor Models • The information received depends on the question asked: • not all models are appropriate for all questions • Drugs need different types of models at different times • in their “discovery / development” life cycle • “Pharmacology” models to qualify compound • “Efficacy” models to define potential for biologic effect • Target driven • Target unselected • “Biology” models to confirm ONLY the target • or molecular events related to target are affected
TARGET-DEPENDENT IN VIVO MODEL IND DIRECTED TOX/FORM PHASE I: DOSE/SCHEDULE: HUMAN PHARM/TOX; ? AFFECT TARGET PHASE II: ACTIVITY = ? AFFECT TARGET PHASE III: SURVIVAL/TIME TO PROGRESSION “Rational” Drug Discovery MOLECULAR TARGET SCREEN PHARMACOLOGY (to affect target) Biochemical Engineered cell Animal (yeast/worm/fish) CHEMISTRY
S G2 G1 M Cell Proliferation Cell Death How To “Build” A Cancer Cell Cancer cells possess defined “families” of lesions with common outcomes • “Misfiring” or Abnormality of Cell Cycle • Imbalance of Genes Regulating Cell Death • Immortality / Telomerase • Angiogenesis / Invasion Phenotype - “Oncogenes” turned on - “Suppressor genes” turned off - Mimic Growth Regulatory “Signal Transduction” G0 Tumor Size (After Varmus, Bishop, Weinberg, Croce, Folkman, Hanahan … etc.)
Molecular Target Definition - How To? • BIOLOGY: • “ RETROFIT” ACTIVE MOLECULES: • “CLASSICAL:” • CHEMICAL GENETICS: * Cytogenetics Breakpoints Molecules (bcr-abl) * “Positive” selection from tumor DNA Active oncogenes (signal transduction) * Tumor gene expression profiling (CGAP) * Binding partners (geldanamycin, rapamycin, fumagillin) * Computational algorithm (molecule target) * Cell metabolism / Cell cycle effects * Suggest single targets Inefficient * Libraries of molecules and precisely defined organisms - COMPARE - Cluster analysis
bcr-abl As Target: Rationale • Apparently pathogenetic in t9:Q22 (Ph+) CML/ALL • Absence in normal tissues • Modulate signal transduction events downstream Maintenance of chronic phase Adjunct to bone marrow transplantation
bcr-abl Fusion Protein DNA Actin bcr SH2 SH2 V SH2/SH3 kinase NT bcr autophosphorylation Phosphorylation of other substances McWhirter JR, EMBO 12:1533, 1993
Example Of “Rational” Approach:bcr-abl directed agents Natural product empiric lead 1st generation synthetic 2nd generation synthetic; in clinic erbstatin lavendustin piceatannol AG957 AG1112 CGP 57148B = STI571
STI571:An Oral In Vivo Bcr-abl Kinase Inhibitor (days) (hrs) (days) Tyr phosphorylation in vivo Antitumor activity in vivo le Coutre et al, JNCI 91:163, 1999
Efficacy And Safety Of A Specific Inhibitor Of The Bcr-abl Tyrosine Kinase In Chronic Myeloid Leukemia 100 100 80 60 10 40 20 1 0 30 60 90 120 150 0 0 100 200 300 400 BRIAN J.DRUKER,M.D.,MOSHE TALPAZ,M.D.,DEBRA J.RESTA,R.N.,BIN PENG,PH.D., ELISABETH BUCHDUNGER,PH.D.,JOHN M.FORD,M.D.,NICHOLAS B.LYDON,PH.D.,HAGOP KANTARJIAN,M.D., RENAUD CAPDEVILLE,M.D.,SAYURI OHNO-JONES,B.S.,AND CHARLES L.SAWYERS,M.D. Ph Chromosome + Cells White Cell Count % in Metaphase (cells x 10-3 / mm3) Duration of Treatment with STI571 (Days) NEJM 344: 1031, 2001
NCI Drug Discovery A Marriage Of Empirical And Rational Opportunities • Aids to find targets / link targets with drugs • -Cancer Genome Anatomy Project (CGAP) • -Developmental Therapeutics Program In Vitro Drug Screen • Where the target is known: build its assessment into the selection and development of a compound: e.g., 17-allylamino 17-demethoxy geldanamycin (17-AAG) • Where the target is unknown, define it or a proximal indicator of effect in parallel with conventional development path: e.g., UCN-01 protein kinase inhibitor
Tumor material (archival) • “Laser capture microdissection” of tumor cells • Creation of tumor-derived cDNA libraries • Sequence to establish uniqueness • Deposit in public domain from defined sections Cancer Genome Anatomy Project: PROCESS
Normal Cell Cancer Cell Gene Expression: The Cell’s Fingerprint Establishing for a cell the repertoire of genes expressed, together with the amount of gene products produced for each, yields a powerful "fingerprint". Comparing the fingerprints of a normal versus a cancer cell will highlight genes that by their suspicious absence or presence (such as Gene H ) deserve further scientific scrutiny to determine whether such suspects play a role in cancer, or can be exploited in a test for early detection. http://cgap.nci.nih.gov
1985 Hypothesis: Emerging Realities: • Cell type specific agents • Activity in solid tumors • Unique patterns of activity, cut across cell types • Correlations of compound activity AND Cell type selective patterns found - relate to molecular “target” expression - generate hypothesis re: molecular target NCI In Vitro Drug Screen
National Cancer Institute Developmental Therapeutics Program Dose Response Curves NSC: 643248-Q/2 (a rapamycin) Exp. ID: 9503SC35-46 All Cell Lines 100 50 0 Percentage Growth -50 -100 -7 -9 -8 -6 -5 -4 Log10 of Sample Concentration (Molar)
resistant mean sensitive Pattern Recognition Algorithm:COMPARE • Goal: COMPARE degree of similarity of a new • compound to standard agents • Calculate mean GI50, TGI or LC50 • Display behavior of particular cell line as deflection • from mean • Calculate Pearson correlation coefficient: 1 = identity ; 0 = no correlation
Agents With Similar Mechanisms HaveSimilar Mean Graphs Leukemia NSCLC Small Cell Lung Colon CNS Melanoma Ovarian Renal Taxol Halichondrin B Daunorubicin Topoisomerase II Tubulin
5FU/DPYD L-Asparaginase /ASNS Drug TargetClusteringsReveal Clues To Mechanism Nature Genetics 24: 236, 2000; http://dtp.nci.nih.gov
benzoquinone ansa ring carbamate NSC R Geldanamycin 17-AAG 122750 330507 OMe NHCH2CH=CH2 Geldanamycin Structure
Effect of 6 hr, 0.35 M herbimycin A on SKBr3 cells % of control Parameter p185 protein p185 Y-P erbB2 RNA Prot syn RNA syn ATP ATP/ADP 35 5 130 84 90 99 108 0 2 4 6 8 Benzoquinoid AnsamycinsInitial Cell Pharmacology • Reduce levels or inhibit transformation by a large number of PTKs: src, yes, fps, erbB1, lck • e.g., 17AAG decrease erbB2 under conditions where overall transcription/translation little affected 150 100 50 0 MDA MB 453 p185 Protein p185 PY % Control Hours (Miller et al, Cancer Res 54: 2724, 1994)
Dose (mg/kg) Drug Deaths % Opt T/C (D) Growth Delay # Schedule 20 6 6 6 0 3.4 2.3 1.5 qd x 5 (9) qd x 5 (9) qd x 5 (9) qd x 5 (9) 0 3 1 0 --- Toxic 33(22) 90(15) --- --- 50 3 DTP, NCI In Vivo EvaluationOf Geldanamycin In PC3 Prostate CA Early Stage, Athymic Mouse Xenograft Route of administration – i.p. Conclude: Narrow therapeutic index on this schedule Solubility of agent major problem for other schedules
18 Atom Spacer Bead Geldanamycin Bead
R. Lysate 1 2 3 4 p90 Geldanamycin BeadsIdentify Hsp90 As Binding Partner 1) Bead-Geld 2) Bead-Geld + Geld 3) Bead-Geld + Geldampicin 4) Bead Neckers et al, PNAS 91:8324, 1994
G0 degradation erbB2 EGFR lck, met, etc X-mRNA X raf ER folding X X hsp 90 nucleus Hsp 90 EIF2 kinase pAKT Immature X Mature X * Cyclin D hsp 90 ER PR etc telomerase nucleus * hsp 90 * hsp 90 Hsp 90 A. C. B.
Three Dimensional View Of Geldanamycin Binding Pocket In Amino Terminus Of Hsp90 Stebbins et al, Cell 89:239, 1997
120 120 100 100 0.03 0.1 0.3 0.5 2 0.03 0.1 0.3 0.5 2 0.03 0.1 0.3 0.5 2 0.03 0.1 0.3 0.5 2 80 80 Raf-1 p185erbB2 control control 60 60 40 40 20 20 (M) 17-AAG GA (M) 17-AAG GA 0 0 17-AAG GA 17-AAG GA 0 0 1 1 10 10 100 100 1000 1000 10000 10000 17-AAG Binds To Hsp90 & Shares Important Biologic Activities With Geldanamycin erbB2 (% of base line) Raf-1 (% of base line) dose (nM) dose (nM) Schulte & Neckers, Cancer Chemother Pharmacol 42: 273, 1998
UCN-01 IC50 Potent antiproliferative agent Cell cycle arrest DNA-damage G2 checkpoint abrogation 37nM 300-600 nM ~50nM (DTP screen)
Chk 1 mediates the G2 checkpoint UCN-01 spRad3(hATM/hATR) Chk1 Chk1-P 14-3-3 Cdc25-P(Ser216) Cdc25-P(Ser216)-14-3-3 Cdc25 Active Active? Inactive Cdc2 Cdc2-P(Tyr15) Active Inactive Adapted from Weinert, Science 277:1450, 1997 Enter mitosis G2 arrest A DNA Damage G2 Checkpoint Is Mediated By CDKs: UCN-01 Action
70 60 50 40 30 20 10 0 70 60 50 40 30 20 10 0 30 40 50 60 0 10 1000 100000 UCN-01 w/o plasma UCN-01 in plasma UCN-01 Infusional Phase I TrialG2 Checkpoint Abrogation % G2 checkpoint abrogation % G2 checkpoint abrogation nM UCN-01 UCN-01 (mg/m2/day)
Challenges In Pursuing TheMolecular Therapeutics Of Cancer • Must change thinking from histologic to molecular • diagnoses (CGAP, array technology) • Develop new means (imaging, probes) to assess • molecular pharmacodynamics • Must move away from cytotoxicity as sole primary • endpoint: assess and evaluate cytostatic effect • Promote patient participation in clinical trials • Develop speed and efficiency in answering critical • clinical questions
Goals For Cancer Drug ScreeningIn The New Millennium • Associate novel chemotypes with defined targets • may utilize purified targets at the “front end” • may define targets in pathway/organisms • may “retrofit” molecules to targets or pathways • by statistical approaches • Allows facile tools for chemical/pharmacological • optimization • Define targets of relevance to and translatable in • early clinical trials
Summary:Developmental Therapeutics Program, NCI • Novel agents directed at molecular targets • important to cancer pathogenesis • and progression • Interdisciplinary collaborators: academia, • industry, intramural NCI • Contribute agents and regimens for use by • intra / extramural investigators
Acknowledgements NCI V. Narayanan, R. Schultz J. Johnson, S. O’Barr M. Hollingshead, S. Stinson L. Rubinstein A.Monks, N. Scudiero K. Paull, D. Zaharevitz, S. Bates S. Holbeck, J. Weinstein A. Senderowicz A. Murgo, S. Arbuck G. Kaur, P. Worland, Q. Wang P. O’Connor L. Neckers, L. Whitesell D. Newman H. Piwnica-Worms Wash U V. Pollack Pfizer M. Roberge U. Brit. Columbia
Our next speaker is: Ms. Shannon Decker Office of the Associate Director Developmental Therapeutics Program