Download
1 / 8
120 likes | 646 Views
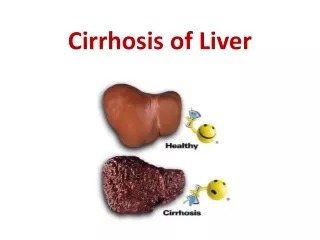
Complications of Liver Cirrhosis. By Samuel Riney Capstone 2014. Cirrhosis. Fibrosis and nodular regeneration Etiology: alcohol and hepatitis are common Liver enlarged at first, shrunken later Sx : jaundice, spider angiomata , palmar erythema Dx : abdominal US w/ Doppler, biopsy.

E N D
Complications of Liver Cirrhosis By Samuel Riney Capstone 2014
Cirrhosis • Fibrosis and nodular regeneration • Etiology: alcohol and hepatitis are common • Liver enlarged at first, shrunken later • Sx: jaundice, spider angiomata, palmarerythema • Dx: abdominal US w/ Doppler, biopsy
4 Main Complications • Ascites • Spontaneous bacterial peritonitis • Gastroesophagealvarices • Hepatic encephalopathy
Ascites • Due to portal hypertension • Develops in 60% w/in 10 years • Tx: • Decreased Na intake • Spironolactone • Furosemide • Refractory ascites- LVP or TIPS
Spontaneous Bacterial Peritonitis • Develops in about 20% • Presents with abdominal pain, encephalopathy • Due to GNR 70%, GPC 30% • Tx: Abx like cefotaxime IV or ofloxacin PO
GastroesophogealVarices • Screen all cirrhotics • Common source of upper GI bleed • Tx: • Nonselective beta blocker • Endoscopic band ligation Courtesy of Wikimedia Commons
Hepatic Encephalopathy • Liver failure to detoxify NH3 • Leads to cerebral edema • Asterixis is common finding • Tx: Lactulose
A 64 y/o gentleman with a history of alcoholic liver disease comes to see you in your primary care clinic. He is new to the area and is looking for a new physician to manage his chronic conditions. In the course of your visit, you note that he has confirmed cirrhosis of the liver with portal hypertension. Upon reviewing his medications, he is taking only spironolactone and furosemide. He has no complaints today. His vital signs are within normal limits today. Physical exam reveals an enlarged liver, slightly distended belly, large dilated superficial abdominal veins, and 2+ pedal edema. A recent EGD confirmed the presence of esophageal varices. After the exam, he states his concerned about the current treatment plan and wants to know if there is anything else he can do to prevent future complications.Which of the following would you most recommend adding to this patients treatment? • Aspirin 325mg • Bactrim • Compression stockings • Hydrochlorothiazide • Propranolol