Download
1 / 18
240 likes | 597 Views
Cerebral Vein Thrombosis. Morning Report Sima Patel 5/13/09. CEREBRAL VEIN and SINUS THROMBOSIS. Thrombosis of the dural venous sinuses and associated veins First described by French physician Ribes in 1825 who observed thrombosis of the saggital sinus and cerebral veins. .

E N D
Cerebral Vein Thrombosis Morning Report Sima Patel 5/13/09
CEREBRAL VEIN and SINUS THROMBOSIS • Thrombosis of the dural venous sinuses and associated veins • First described by French physician Ribes in 1825 who observed thrombosis of the saggital sinus and cerebral veins.
EPIDEMIOLOGY • 3-4 cases per million in adults • Most common in 3rd decade of live • 75% are female • Older studies show no difference in gender and it is believed that use of oral contraceptive have played a role • Accounts for 50% of strokes during pregnancy and peripartum period
RISK FACTORS • Thrombotic disorders • Factor V leiden • Protein C deficiency • Protein S deficiency • Antithrombin III deficiency • Antiphospholipid syndrome • Lupus anticoagulant
RISK FACTORS • Nephrotic syndrome • Chronic inflammatory diseases such as IBD (felt to be mediated by endotoxins and abnormalities of the fibrinolyticsystem, platelet count and functions) • Collagen vascular diseases – Lupus, Wegeners, Behcet syndrome • Hyperhomocysteinemia
RISK FACTORS • Pregnancy and peripartum period • Polycythemia Vera • Paroxysmal NocturalHemoglobinuria • Oral Contraception use (estrogen containing) • Infection - Meningitis, otitis media, sinusitis, mastoiditis • Direct injury to the venous sinuses
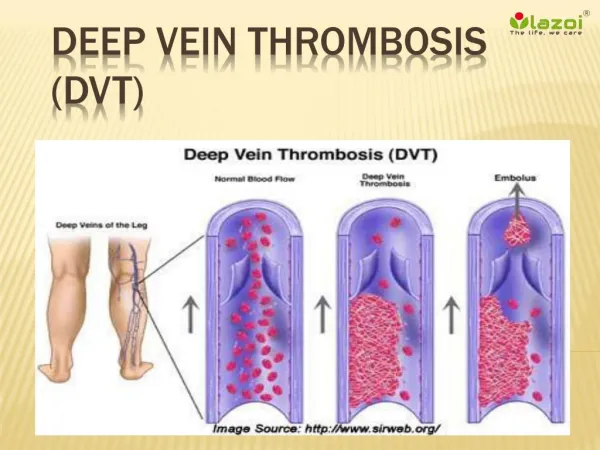
PATHOGENESIS • Formation of blood clots in the veins aswell as venous sinuses of the brain • Thrombosis of the veins cause infarcts to associated brain tissue and can result in cerebral edema. • Infarcts can lad to hemorrhages (40% can progress to hemorrhagic infarcts) • Sinus thrombosis leads to decreased resorption of the CSF leading to increased intracranial pressure • Most cases of cerebral venous sinus thrombosis are due to hypercoagulability • Thrombosis can lead to embolization and PE (occurs in 10% of patients)
CLINICAL PRESENTATION • Headache (sudden or gradual) – in 90% of patients • Symptoms of stroke – in 50% of patients • Seizures (usually affect only one part of the body) – in 40% of patients • AMS • Increased intracranial pressure visual changes • If cavernous sinus thrombosis (3%) then can present with proptosis and painful ophthalmoplegia • Other: nausea/vomiting, vestibular neuropathy, pulsatile tinnitus, double vision, unilateral deafness, facial weakness, visual changes
EVALUATION • CBC • Antiphospholipid and anticardiolipin antibodies • Protein S • Protein C • Antithrombin III • Lupus anticoagulant • Factor V Leiden • Hb Electrophoresis • ESR • ANA • Urine protein • LFT
DIAGNOSIS • Based on symptoms (headache, signs of increased ICP, neurologic deficits) • CT • MRI • Angiography – may be able to demonstrate smaller clots than MRI and CT • Most sensitive MRI and MRV
TREATMENT • Heparin or low molecular weight heparin for initial treatment followed by coumadin • If extensive hemorrhage, repeat imaging in 7-10 days to determine if anticoagulation safe. • If thrombosis occurred under temporary conditions, the patient will need 3 months of anticoagulation
TREATMENT • If no clear cause or condition unprovoked then needs 6-12 months anticoagulation • If underlying thrombotic disorder then needs lifelong anticoagulation • Thrombolysis is restricted to those with a poor prognosis
PROGNOSIS • Mortality 5.6% during hospitalization • Mortality 50% in children • 88% have total or near complete recovery • Rate of recurrence 2.8%
REFERENCES • Ida Martinelli, Sacchi E, Landi G, Taioli E, Duca F. High Risk of Cerebral Vein Thrombosis in Carriers of Prothrombin-Gene Mutation and in users of Oral Contraceptives. New England Journal of Medicine June 18, 1998; Volume 338: 1793-1979 • Prakash C, Bansal BC. Cerebral Venous Thrombosis. Journal of Indian Academy of Clinical Medicine. • www.uptodate.com