Download
1 / 40
500 likes | 2.35k Views
Hypotonia - the floppy baby. SMA Spinal Muscular Atrophy. הצגת מקרה – מ.ג'. נולדה בשבוע 42 לאחר הריון תקין, בלידה - מים מקוניאלים אפגר 1 דק' -7 , 5 דק' - 9 משקל לידה -3030, היקף ראש – 34.5 במשפחה – הורים בני דודים דרגה ראשונה, לא ידוע על מחלות. אח בן 5 – איחור התפתחותי על רקע לא ברור.

E N D
Hypotonia - the floppy baby SMA Spinal Muscular Atrophy
הצגת מקרה – מ.ג' • נולדה בשבוע 42 לאחר הריון תקין, • בלידה - מים מקוניאלים • אפגר 1 דק' -7 , 5 דק' - 9 • משקל לידה -3030, היקף ראש – 34.5 • במשפחה – הורים בני דודים דרגה ראשונה, לא ידוע על מחלות. אח בן 5 – איחור התפתחותי על רקע לא ברור.
הצגת מקרה – מ.ג' • בבדיקה גופנית : • היפוטוניה בולטת. • לא הופקו החזרים גידיים. • בכי חלש. • יש מציצה. • נשימה בעיקר סרעפתית. • נצפו פסיקולציות בלשון. • עירנית, עוקבת עם תגובות ראיה ושמיעה טובות.
הצגת מקרה – מ.ג' • בירור שבוצע: • במעבדה : CPK מוגבר – 1180 • אקו לב – PDA ו PFO קטן : בגדר הנורמה ליום 2 של חיים. חדרים בגודל תקין, התכווצות תקינה. • בדיקת עיניים – תקינה • US מוח – תקין • EMG – סימני דהנרווציה במידה בינונית • בדיקה גנטית – SMA type 1
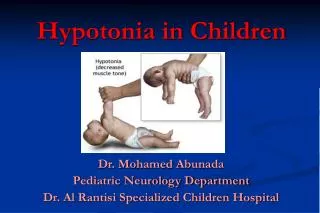
Hypotonia in the newborn • Almost any condition that affects the central or peripheral nervous system can be expressed by a reduction of tone. • Most acute or multisystem illness in neonated is accompaied by some degree of hypotonia therefore: sepsis, organ failure, metabolic dysfunction or other systemic illness must be ruled out.
Diagnosis - Hx • Detailed family, obsteteric, and delivery history. • Polyhydramnios • Decrease in fetal movement • Malpresentation • Birth trauma / Asphyxia
Diagnosis – Phys. exam. • General appearance • Skin – pallor, trauma, bruising, petechias • Dysmorphic features, Weight, length and head size and shape, Respiratory – rate, pattern, Cardiovascular, Organomegaly, Genitalia, cotractures • Neurologic examination – alertness, fixes or follows, posture and spontaneous movements, cranial nerves – eye movements, fisting, abnormal primitive reflex, character of deep tedon reflexes (upper vs lower), sensation, ability to suck ad swallow, character of cry, tongue fasciculations
SMA –spinal muscular atrophy • The spinal muscular atrophies (SMAs) are characterized by degeneration of the anterior horn cells in the spinal cord and motor nuclei in the lower brainstem.
HISTORY • Was first described in the 1890s by Guido Werdnig of the university of Viena and Johann Hoffmann of Heidelberg University.
Frequency: • The acute infantile-onset SMA (type I) affects approximately 1 per 10,000 live births. • The chronic forms (types II and III), 1 per 24,000 births
Clinical features – TYPE 1 • Werding Hoffman / infantile onset SMA • Weakness and profound hypotonia – first few months of life • Normal social awareness and interaction • Limited spontaneous movement • Deep tendon reflexes are absent • Sphincter tone and sensation are intact
Clinical features – TYPE 1 • Muscle trembling can be seen in fingers and fasciculitations are often present in the tongue • Pectus excavatum and flaring of the lower ribs (weak intercostal muscles) • Feeding difficulties – FTT • Aspiration • Rarely survive beyond 2 yrs
Clinical features – TYPE 2 • Milestones are usually normal until onset – 6-18 months. • Legs are weaker then arms – failure to walk • Deep tendon reflexes – variable pattern • Usually sit without support, some walk with bracing • Survive into adolescence and beyond • Good pulmunary function
Clinical features – TYPE 3 • Kugelberg-Welander disease • Independent ambulation acheived • Normal survival • Onset of weakness after 18 mo – often late childhood or adolecence • Waddling gait with lumbar lordosis • Decrease in motor units over time has been documented (despite clinical picture)
Diagnosis • Clinical, physical exam, family Hx • Lab: • CK level is usually normal in SMA type I and normal or slightly elevated in the other types • Cerebrospinal fluid findings are normal • Genetic testing, both prenatally and postnatally
Diagnosis • Nerve conduction studies – normal or slightly decreased velocities, the sensory nerve action potentials are normal. • Electromyography – abnormal spontaneous activity with fibrillations and positive sharp waves. The mean duration and amplitude of motor unit action potentials are increased.
Histology • Muscle biopsy: large groups of circular atrophic type 1 and 2 muscle fibers intersperseded among fascicles of hypertrophied type 1 fibers. The enlarged fibers have been reinnervated by the sprouting of surviving nerves and are 3-4 times larger than normal.
Genetics • Autosomal recessive disorder caused by homozygous deletions or mutations of the SMN1 gene at the 5 q11 locus. • There are two copies of the smn gene on chrom. 5q that code for SMN protein – SMN1 and SMN2.
Genetics • All SMA patients have reduced fl-smn protein : • Type 1 – 9% • Type 2 – 14% • Type 3 – 18% • Carriers – 45 -55% • When levels approach 23% - motor neuron function is normal.
Genetics • SMA type I: Mutations • Mostly SMN1 deletions • Few missense point mutations in SMN1 • SMN2 gene copy number: Often 2 • SMA type II • Mutations convert SMN1 gene to SMN2 • SMN2 gene copy number: > 3 • Missense point mutations more common • SMA type III • SMN2 gene copy number: > 3 • Missense point mutations more common
SMN protein • Expressed in most tissues • High levels are found in spinal motor neuron • SMN exist in the cell as a part of a large complex that regulates the assembly of a specific class of RNA protein complexes - which is essential for pre-mRNA splicing. • The function of SMN protein is linked to the control of protein synthesis.
The Role of SMN in SMA -1 • SMA is a direct consequence of a defect in pre-RNA splicing: • The affected motor neurons, being large, high energy requiring cells, have a lower tolerance for depleted SMN levels and are uniquely sensitive.
The Role of SMN in SMA - 2 • SMA is a consequence of a motor neuron specific function of the SMN protein: • From observations demonstrating the accumulation of the SMN protein in the axons and growth cones of neuron like cells in vitro and anterior horn cells in vivo.
Potential for Therapies • The disease phenotype is proportional to the amount of fl-SMA. • Mechanisms for potential therapies: • Enhanced expression of SMN2 • Altering SMN2 transcript splicing to increase the level of fl-SMN RNA • Other strategies to increase the level or activity on SMN.
Potential for Therapies • In was found that histone deacetylase (HDAC) inhibitors can increase the level of fl-SMN. • Studies with other agents also show promise – sodium butyrate, valproic acid.
הצגת מקרה – מ.ג' • כעת בת חודשיים וחצי. • שלושה אשפוזים במחלקתינו: • דלקת ריאות ימין (אספירציה?) • ירידה ביכולת אכילה ובמצבה הכללי – שוחררה לביתה עם זונדה. • דלקת ריאות ימין על רקע אספירציה, התדרדרות נשימתית, שוחררה עם חמצן. • מוגדרת DNR