Download
1 / 30
310 likes | 1.03k Views
ECG Interpretation. Arrhythmias of Formation Chapters 4-5. Types of Arryhthmias:. Sinus Problems: Formed in the sinus node, but irregular Ectopic Problems: Formed outside of the sinus node Conduction Problems: Formed in the sinus node, but conduction in error

E N D
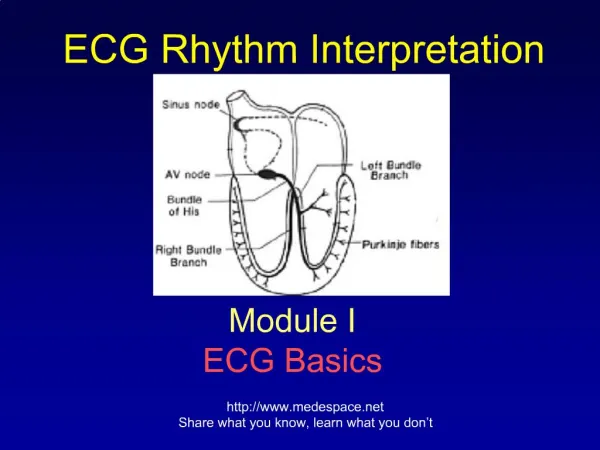
ECG Interpretation Arrhythmias of Formation Chapters 4-5
Types of Arryhthmias: • Sinus Problems: Formed in the sinus node, but irregular • Ectopic Problems: Formedoutside of the sinus node • Conduction Problems: Formed in the sinus node, but conduction in error • Pre-Excitation Problems: “Short circuits” in normal conduction
Causes of Arrhytmias: • Hypoxia: Lung disease • Ischemia: CAD, angina (local hypoxia) • Sympathetic Stimulation: Nervous, exercise, CHF, hyperthyroidism • Drugs: Caffeine, cocaine, stimulants…many antiarryhtmic drugs… • Electrolyte Disturbances: K+, Ca++, Mg++ • Bradycardia: “Escape” rhythms… • Stretch: CHF, hypertrophy, valve disease
Rhythm ID: Algorithm • P-Wave: rate and rhythm • QRS: rate and rhythm - shape • P-R Interval: Is AV conduction normal? P:QRS regular? • T Wave and QT Interval • Any unusual complexes? • IS IT DANGEROUS?
Clinical Manifestations: • Asymptomatic – generally benign • Palpitations – Awareness may cause anxiety • Compromised CO – Syncope • Myocardial Ischemia – tachy • CHF – Chronic insufficiency • Sudden Death – Cardiac arrest
Define “Normal” • Regular Atrial and Ventricular Rhythms: 1P : 1 QRS • Rates: 60-100 • P Morphology: small, round, regular and positive in Lead II • QRS Morph: Similar size and shape • Positive T waves in Lead II
P-Wave: • 1.SA Node “fires” • 2. Right and Left Atria Depolarize • 3. AV Node “pauses” • Questions: • P waves present? • Regular rhythm? • 1/QRS? AV Node SA Node LA/RA Depol
Sinus Rhythms • Normal Sinus Rhythm: 1P/QRS: 60-100 bpm • Sinus brady: 1P/QRS: <60 bpm • Sinus tachy: 1P/QRS: >100 bpm • Sinus Arrhythmia: 1P/QRSNormalIrregularities caused by inspiration/expiration – more noticeable in children / elderly
ABSENT PQRS Complex: Sinus Arrest: • Causes: • Heart disease, acute infection, VAGAL stimulation (Bush’s Pretzel Problem?) • Sick Sinus Syndrome: Usually in elderly – more irregular • DANGER? • Rare and asymptomatic • Frequent and symptomatic
Atrial Arrhythmias: • PAC: Premature Atrial Contraction • Atrial Tachycardias: SVT – with or without blocks, PAT • Atrial Flutter: • Atrial Fibrillation
Premature Atrial Contractions: • Ectopic • Triggered by: Alcohol, nicotine, anxiety, fatigue, fever, and infections • Usually benign • Clinical Manifestations: Palpitations or “skipped beats”
PAC - ID: • Irregular P-R rhythms • Premature, irregular P waves (sometimes “lost” in the T wave)
Atrial Tachycardias: • Also: Supra Ventricular Tachycardia (PSVT) • Rates: 100-250 bpm • Regular Rhythms • “Hidden” P waves (could be inverted – indicating a Junctional focus PSVT) • PAT = Common in warm-up/cool down and doesn’t respond to Carotid Massage (don’t try this!)
Atrial Flutter: 2:1 Ventricular “capture” Ventricles can only respond to every other Atrial conduction
Multi-focal origins -chaotic Rate: >400 bpm IRREGULAR-R Atrial Cardiac Output is lost : One focus - organized Rate: 200-400 bpm Atrial Cardiac Output is compromised Fibrillation vs. Flutter? Atria contribute ~20% of the total Cardiac output: A-Fib is non-lethal
Summarize: Sinus and Atrial Rhythms • Sinus: Normal, Tachy, Brady • Absent P: Sinus Arrest, A-fib, Junctional (PSVT), PAT • Weird P: A-Flut, PAC
Formation Arrhythmias Junctional and Ventricular Chapters 6-7
Junctional: • Form in the AV (Junction) Node • May be an “Escape” rescue if SA node fails to fire or conduct • Escape Rate ~40-60 bpm • May be an “Ectopic” Irritable Focus • Ectopic Rate ~ 60-100 bpm • Responds to vagal stimulus • P Waves inverted, missing or after the QRS
Ventricles: QRS Rhythms • Regular rhythms? • R-R intervals equivalent • Regular “irregular” rhythms? • R-R intervals equivalent with occasional irregularities • Irregular rhythms? • R-R intervals irregular
Regular “Irregular” • Premature Beats: PVC • Widened QRS, not associated with preceding P wave • Usually does not disrupt P-wave regularity • T wave is “inverted” after PVC • Often Followed by compensatory ventricular pause
PVC Patterns: • PVC: 1 Isolated beat • Couplet: 2 consecutive PVC’s • Bigeminy: PVC every other beat • Non-Sustained VT: >3 beats for less than 1 minute • Sustained VT: > 1 minute of ventricular tachycardia
Irregular Ventricular Rhythms: CHAOTIC • Ventricular Fibrillation: • Multi-focal origins • Irregular wave morphologies • Cardiac Output = 0 • Coarse vs. Fine V-Fib
Clinical Manifestations – PVC’s • Often benign BUT • Compromised CO • Possibly precipitate a lethal arrhythmia: Vtach, VFib
More on PVC’s • Cardiac Output: Pulse deficit = reduced CO (~20%) • One PVC usually asymptomatic • Symptoms: LOC or dizziness demand treatment • Risk of Lethal Arrhythmias: V-Tach more dangerous in CAD
Rules of Malignancy: • Frequency: > 6 / minute • Runs: 3+ consecutive • Multiform • “R on T” • PVC’s during MI
What is the threat of sustained Ventricular Tachycardia?1. What happens to diastole? 2. What happens to Cardiac Output? 3. What happens to myocardial perfusion?4. What happens to myocardial VO2?