Download

1 / 34
450 likes | 1.73k Views
Atrial fibrillation June 2006 Changing clinical practice NICE guidelines are based on the best available evidence The Department of Health asks NHS organisations to work towards implementing guidelines Compliance will be monitored by the Healthcare Commission Atrial fibrillation

E N D
Atrial fibrillation June 2006
Changing clinical practice • NICE guidelines are based on the best available evidence • The Department of Health asks NHS organisations to work towards implementing guidelines • Compliance will be monitored by the Healthcare Commission
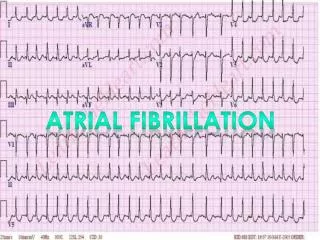
Atrial fibrillation • Atrial fibrillation (AF) is an atrial tachyarrhythmia characterised by predominantly uncoordinated atrial activation with consequent deterioration of atrial mechanical function • On the ECG, there is an absence of consistent P waves; instead there are rapid oscillations or fibrillatory waves that vary in size, shape and timing
Reproduced by kind permission of Ashford and St. Peter’s Hospitals NHS Trust
Several causes of AF • Often caused by co-existing medical conditions – both cardiac and non-cardiac • Associated with increasing age, hypertension, heart failure, diabetes mellitus and valve disease • Dietary and lifestyle factors have also been associated with AF • Common after surgery, especially cardiothoracic operations
Need for this guideline • AF is a significant risk factor for mortality, as well as stroke and other morbidities • AF is the commonest sustained cardiac arrhythmia • Too often, AF is detected only after the patient presents with serious complications of AF • AF incidence and prevalence increase with increasing age. With an increasingly elderly population, AF is likely to become more common
Commonest cardiac arrhythmia • The prevalence of AF roughly doubles with each decade of age: from 0.5% at age 50–59 years to almost 9.0% at age 80–90 years • Present in 3–6% of acute hospital admissions • Prevalence of 4.7% of people aged 65 years or over in general practice
Prevalence of AF in the Renfrew-Paisley study Cohort of men and women aged 45–64 years (n = 15,406) Reproduced with permission of the BMJ Publishing Group from Stewart S et al, Heart 2001: 86:516-21
What needs to happen • Opportunistic/targeted case detection including taking a manual pulse to detect AF • Accurate diagnosis of AF using an ECG • Further investigations and clinical assessment, including risk stratification for stroke/thromboembolism • Development of a management plan – rate-control, rhythm-control or referral • Antithrombotic therapy as appropriate • Follow-up and review
Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up AF care pathway The management and presentation of AF involves all healthcare settings Primary/secondary/ emergency care Primary/secondary care Secondary/tertiary care
Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up Key priority – detection and diagnosis An ECG should be performed in all patients, whether symptomatic or not, in whom AF is suspected because an irregular pulse has been detected
Suggested actions • People with undiagnosed AF can receive treatment sooner if opportunistic case finding is undertaken using manual pulse palpation • Promote opportunistic case detection and targeting of patients at increased risk: • Primary care: appropriate long-term condition registers, people aged >65 years, flu vaccination programme • Secondary care: A&E, outpatient clinics and wards, especially care of the elderly
Suggested actions • Remember to use ECG to confirm diagnosis and the routine recording of ECG results • Review access to diagnostics – irrespective of how services are structured locally, easy access and rapid reporting are essential • Remember incentives and encourage practices to establish and maintain a practice-based AF register in line with the QOF 06/07 AF indicators • Consider establishing a PCT-led, community-based, rapid-access arrhythmia clinic
Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up Key priority – choosing the most effective treatment • Some patients with • persistent AF will satisfy • criteria for either an initial • rate- or rhythm-control • strategy • Indications for each • option are not mutually • exclusive • Involve the patient in the • treatment decision • Take comorbidities into • account • Antithrombotic therapy • should always be used
Treatment for persistent AF • Two main treatment strategies: • Rate-control involves the use of chronotropic drugs or electrophysiological/surgical interventions • Rhythm-control involves the use of electrical or pharmacological cardioversion for persistent AF, or suppression of recurrent (e.g. paroxysmal) AF • There is still the need for appropriate antithrombotic therapy if a rhythm-control strategy is chosen
Rate-control strategy • Try rate control first for patients with persistent AF: • over 65 • with coronary artery disease • with contraindications to antiarrhythmic drugs • unsuitable for cardioversion • without congestive heart failure
Rhythm-control strategy • Try rhythm-control first for patients with persistent AF: • who are symptomatic • who are younger • presenting for the first time with lone AF • secondary to a treated/corrected precipitant • with congestive heart failure
Suggested actions • Liaise with your local cardiac network – benefit from shared learning and support. For example, some areas have established a primary care rapid access arrhythmia clinic and the provision of an arrhythmia care co-ordinator or an arrhythmia nurse specialist • Provide awareness raising and education sessions for healthcare professionals – don’t forget to include out-of-hours services • Develop, promote and disseminate quality patient information and decision aids for clinicians
Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up Key priority – assess for risk of stroke and thromboembolism • Use the ‘stroke risk • stratification algorithm’ to • assess risk of stroke and • thromboembolism • Use antithrombotic • therapy as appropriate • Initiate antithrombotic • therapy with minimal • delay in patients newly • diagnosed with AF
Patients with AF Determine stroke/thromboembolic risk • High risk: • Previous ischaemic stroke/TIA or thromboembolic event • Age >75 with hypertension, diabetes or vascular disease • Clinical evidence of valve disease, heart failure, or impaired left ventricular function on echocardiography • Moderate risk: • Age >65 with no high risk factors • Age <75 with hypertension, diabetes or vascular disease • Low risk: • Age <65 with no moderate or high risk factors
Patients with AF Determine stroke/thromboembolic risk Low risk High risk Moderate risk Consider anticoagulation Consider anticoagulation or aspirin Aspirin 75 to 300 mg/day if no contraindications Contraindications to warfarin? YES NO Reassess risk stratification whenever individual risk factors are reviewed Warfarin, target INR = 2.5 (range 2.0 to 3.0)
Anticoagulation • Assessment of bleeding risk should be part of the clinical assessment of AF patients prior to starting anticoagulation • Antithrombotic benefits and potential bleeding risks of long-term coagulation should be explained and discussed with the patient • Aim for a target INR of between 2.0 and 3.0 • Forms of monitoring include point of care or near patient testing and patient self-monitoring
Suggested actions • Review anticoagulation services locally • Remember incentives for anticoagulation monitoring and near patient testing, e.g. QOF 06/07 and National Enhanced Services • Provide awareness raising and education sessions - emphasise stroke prevention and promote the use of the stroke risk stratification algorithm • Consider integrating risk stratification into computerised patient management software • Ensure provision of quality patient information
Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up Key priority – optimise pharmacological management In patients with permanent AF, who need treatment for rate-control: – beta-blockers or rate-limiting calcium antagonists should be the preferred initial monotherapy in all patients – digoxin should only be considered as monotherapy in predominantly sedentary patients
Treatment for permanent AF • The aim of heart rate control is to: • minimise symptoms associated with excessive heart rates • prevent tachycardia-associated cardiomyopathy • Digoxin monotherapy should only be useful for older, sedentary patients • Perform a risk–benefit assessment to inform the decision of whether or not to give antithrombotic therapy
Suggested actions • Work with local Drugs and Therapeutics Committees and prescribing advisors to review and update prescribing formularies • Emphasise clinically effective alternatives to digoxin to PCT prescribing advisors and prescribing leads • Provide awareness raising and updating sessions for local primary and secondary care healthcare professionals
Cardioversion • Cardioversion is performed as part of a rhythm-control treatment strategy • There are two types of cardioversion: electrical (ECV) and pharmacological (PCV) • Cardioversion of AF is associated with increased risk of stroke in the absence of antithrombotic therapy • Not all attempts at ECV or PCV are successful • Patient choice is important
Treatment for paroxysmal AF • Patients with paroxysmal AF can be highly symptomatic • Three main aims of treatment for paroxysmal AF are to: • suppress paroxysms of AF and maintain sinus rhythm • control heart rate during paroxysms of AF • prevent complications • Treatment strategies include out-of-hospital initiation of antiarrhythmic drugs: ‘pill in the pocket’ approach • Patients with paroxysmal AF carry the same risks of stroke and thromboembolism as those with persistent AF
Acute-onset AF • Acute-onset AF requires immediate hospitalisation and urgent intervention • Those at highest risk have a ventricular rate greater than 150 bpm, ongoing chest pain or critical perfusion
Follow-up and referral • Follow-up after cardioversion should take place at 1 month, and the frequency of subsequent reviews should be tailored to the patient • Reassess the need for anticoagulation at each review • Referral for further specialist intervention should be considered in patients: • in whom pharmacological therapy has failed • with lone AF • with ECG evidence of any underlying electrophysiological disorder
Costs and savings • Main elements identified as: • costs incurred due to increased use of ECG to confirm diagnosis • increases in the use of anticoagulants in those with AF, which includes: costs of additional anticoagulant services and of major bleeds incurred, and savings resulting from strokes and deaths avoided
Access tools online • Costing tools • costing report • costing template • Audit criteria • Implementation advice • Available from: www.nice.org.uk/cg036
Access the guideline online • Quick reference guide – a summary www.nice.org.uk/CG036quickrefguide • NICE guideline – all of the recommendations www.nice.org.uk/CG036niceguideline • Full guideline – all of the evidence and rationale www.nice.org.uk/CG036fullguideline • Information for the public – a plain English version www.nice.org.uk/CG036publicinfo