Download
1 / 29

E N D
1. Anti-thyroid drug and ANCA positive vasculitis JCEM, vol84, No1, p13, 1999
3. Clinical manifestation 27 year-old female
Thyroid goiter for 3 years.
Follow up at OPD regularly.
91-8-12,
C.C.:Thyroid goiter, palpitation(120/min), hand tremor for several weeks.
PE:goiter, tachycardia, no exophthalmos
5. Thyroid sonogram 87-9-16: Multiple nodular goiter, bilateral , R/O autoimmune thyroiditis
88-8-5: Ditto
89-7-11:in favor of MNG rather than autoimmune thyroid disease.
90-1-1:MNG
90-12-27: atypical MNG
91-7-23: more favor autoimmune thyroid disease, D/D include MNG.
8. 91-8-12,
Inderal and Tapazol were prescribed.
9. Clinical manifestation 91-8-21, acute nuchalgia for 2 days with fever off and on.
PE:
HA: negative, photophobia: negative
Neck : not rigid, no meningeal sign,
BT : 38.5 c, Multiple small petechiae over ??,
Dx: R/O dengue fever.
Admission
17. ANCA positive vasculitides Wegener's granulomatosis (WG),
Churg-Strauss syndrome (CSC)
Microscopic polyangiitis, (MP)
some drug-induced vasculitides.
18. ANCA pericytoplasmic (pANCA)
directed against a number of antigens
the most important -- myeloperoxidase (MPO-ANCA)
Most patients with CSS or MP are pANCA and MPO-ANCA positive cytoplasmic (cANCA)
strongly associated with for antiproteinase3 (PR3-ANCA)
90% WG are PR3-ANCA and cANCA positive
cANCA is 80-97% specific for WG
Drug-induced ANCA positive vasculitis
may be associated with pANCA, MPO-ANCA, cANCA or PR3-ANCA
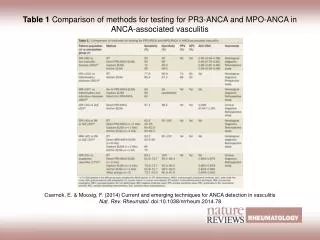
20. Analysis of cases There are 26 previously reported cases of ANCA positive vasculitis in association with antithyroid drugs ( Table 1).
Seventy-four percent were female.
Forty-eight percent were Japanese patients.
The average age of affected patients was 46.6 years (range 8 to 82 years of age).
PTU therapy was implicated in 88%.
Underlying disease
63%was not clear from the case report,
in all but one of the remainder was Graves'.
JCEM, 1999,
21. Organ involvement Renal involvement-- 66.7%,
arthralgia in 48%,
fever in 37%,
skin involvement in 29.6%,
respiratory tract involvement in 25.9%,
myalgia in 22.2%,
scleritis in 14.8%
other manifestations in 18.5%.
22. Renal biopsy 17 patients was done
Crescentic or necrotizing GN in 94.1%.
Mesangial proliferation in 11.8%.
Immunofluorescence test�
pauci-immune
or non-specific in all biopsies.
23. Analysis of cases pANCA pattern--81.5%,
an undifferentiated positive ANCA was reported in a further 14.8%.
cANCA was positive in 11.1% and was seen in isolation in one patient.
MPO-ANCA was positive in 78.3% of cases
PR3-ANCA was positive in 72.7% of the 11 cases
24. Therapy Cessation of the initiating drug.
Renal involvement
steroids and /or
cyclophosphamide was given to 88.2% patients
Plasmapheresis-One patient
25. Result Improvement in 85.2%.
In 7.4%, renal function declined
In 3.7%, no significant change
Death occurred in a patient in whom renal function was stable and was due to LVF and COAD.
26. Discussion Vasculitis is a rare complication during treatment of thyro�toxicosis
Positive ANCA in association with the vasculitis has been recently described
Antithyroid drugs related ANCA vasculitis
more frequently in women, reflect female preponderagce of thyrotoxicosis
In fact men be more common
27. ANCA associated vasculitis a variety of constitutional symptoms
fever,
myalgia,
arthralgia,
"flu-like" syndrome
28. ANCA associated vasculitis Vessels in skin, kidneys, respiratory tract, skeletal muscle, peripheral nerves and other areas may be involved.
29. ANCA associated vasculitis The commonest cutaneous lesion is leukocytoclastic vasculitis
preferentially affects the lower limbs
typically causes purpuric lesions.
Other cutaneous manifestations are protean.
30. ANCA associated vasculitis pathogenesis not clearly understood.
PTU accumulate in neutrophils
bind to myelo�peroxidase,
changing its structure
autoantibody formation
31. Pathogenesis The pauci-immune or non-specific pattern of immunofluorescence in renal biopsies implies that drug-induced lupus erythematosis is unlikely to be the mechanism.
32. Drug-induced pANCA vasculitis hydralazine,
sulpha�salazine therapy (n=2)
minocycline (n=1)
Diagnosis requires a positive ANCA.
MPO-ANCA is the commonest pattern.
Biopsies from clinically involved area.
If renal involvement? renal biopsy ?determining appropriate therapy and long term prognosis.
33. Drug-induced pANCA vasculitis Diagnosis �
positive ANCA.
MPO-ANCA is the commonest pattern.
Biopsies from clinically involved area.
If renal involvement? renal biopsy ?determining appropriate therapy and long term prognosis.
34. Drug-induced pANCA vasculitis Treatment
depends upon severity of the illness.
Fever, arthralgia, myalgia, malaise, "flu-like" syndrome and cutaneous vasculitis respond well to cessation of the drug.
35. Treatment Steroids and/or cyclophosphamide is warranted --If renal manifestation are severe, rapidly progressive, or biopsy shows, crescentic GN,.
In most cases, renal function will improve, but creatinine clearance sometimes does not return to baseline
36. Drug-induced pANCA vasculitis Crescentic or necrotizing GN-- high risk for CRI
Pulmonary manifestations
from minor nasal involvement to life-threatening pulmonary haemorrhage.
If severe or life-threatening,
plasmapheresis should be considered, in addition to steroids and/or cyclophosphamide.
Scleritis --either topical or systemic steroids.
37. Drug-induced pANCA vasculitis Prognosis is good.
ANCA titers may fall with time, but remain positive in many patients.
We found several ANCA positive patients treated with either PTU or carbimazole without clinical manifestations of vasculitis (unpublished data).
39. Conclusion ANCA positivity may lead to
earlier consideration of definitive therapy.
Possibly long-term anti�thyroid therapy should not be given to patients with positive ANCA,
carbimazole should be better than PTU.