Download
1 / 31
390 likes | 1.68k Views
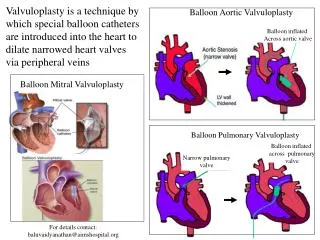
2009 Pediatric and Congenital/Structural Fellows Course. Balloon Aortic Valvuloplasty in Infants and Children. Thomas K. Jones, MD Professor, Pediatrics and Medicine University of Washington School of Medicine Director, Cardiac Catheterization Laboratories Seattle Children’s Hospital.

E N D
2009 Pediatric and Congenital/Structural Fellows Course Balloon Aortic Valvuloplasty in Infants and Children Thomas K. Jones, MD Professor, Pediatrics and Medicine University of Washington School of Medicine Director, Cardiac Catheterization Laboratories Seattle Children’s Hospital
Disclosures 2009 Pediatric and Congenital/Structural Fellows Course • None related to this presentation
History • First reported by Lababidi in 1984* *Lababidi Z, Wu JR, Walls TJ. Percutaneous balloon aortic valvuloplasty: results in 23 patients. Am J Cardiol 1984:53;194-197 • Significant adverse event rate in early reports • Femoral arterial injury • Aortic regurgitation • Death • Major life threatening complications related to age** • 11/204 (5%) • Death in 5/11 less than 1 year old **Rocchini AP, Beekman RH, Shachar GB, Benson L, Schwartz D, Kan JS. Balloon Aortic Valvuloplasty: Results of the Valvuloplasty and Angioplasty of Congenital Anomalies registry. Am J Cardiol 1990:65;784-789 • Operator experience and catheter technology key contributors to improving outcomes
Evolution of Technique • Recognition that initial balloon:annulus ratio = .80-.90 • Importance of meticulous management of guidewire to avoid LV perforation • Low profile balloons • Retrograde approach • Rapid ventricular pacing
Aortic Insufficiency • Increased risk with larger balloon:annulus ratios • Increased risk with young age* • Increased risk with bicuspid, asymmetrically thick valves • Increased risk with time *Fratz S, Gildein HP, Balling G, Sebening W, Genz T, Eicken A, Hess J. Aortic valvuloplasty in pediatric patients substantially postpones the need for aortic valve surgery. A single center experience of 188 patients after up to 17.5 years of follow-up. Circulation 2007;117:1201-1206
Seattle Children’s Hospital approach to severe AS in newborns and infants* • Beginning in 1993 we adopted a uniform policy of performing BAV as the initial treatment for all newborns and infants with severe or critical aortic stenosis. • After this time no surgical valvotomies were performed as the initial intervention *Jones TK, Johnston TA, Rosenthal GL, Duncan BW, Lupinetti FM, Balloon aortic valvuloplasty in neonates and young infants; immediate results, mid-term outcome, predictors of success and need for reintervention. Presented at the 50th Annual Scientific Session, American College of Cardiology, Orlando, FL March 20, 2001
Methods • Retrospective review of medical records, cath lab & surgical data base and echocardiograms • All patients treated by BAV are included
Demographics • 45 patients treated between 4/93 & 4/00 • 11/45 were PDA dependent (PGE infusion) • Age: 0 - 58 (36) days (21 < 7 days) • Weight: 1.1 - 6.3 (3.5) kg • 36/45 (80%) male
Procedure • Percutaneous femoral approach 43/45 • Umbilical arterial approach 2/45 • Aortic annulus dimension determined from lateral aortic or LV angiogram • Initial balloon diameter: 80 - 90 %
Cath Results • BAV successfully performed in all patients • Aortic annulus = 7 + 1 (4.6 - 8.5) mm • Balloon diameter = 7 + 0.9 (5 - 9) mm • Balloon/Annulus = .99 + .11 (.85 - 1.15)
Gradient Reduction p < .001
Complications • 2 major events • 1 umbilical artery hematoma (1 kg premature newborn) • 1 mitral valve tear requiring repair • 6 minor events • 1 VF, spontaneous conversion to NSR • 5 persistent reduced pedal pulses requiring heparin or thrombolytic Rx (4/5 < 1998) • No transfusions
Associated Lesions • 9 Coarctation Aorta (5 repaired pre-BAV, 4 post-BAV) • 1 Interrupted Aortic Arch (repaired pre-BAV) • 1 VSD requiring repair • 1 Severe Mitral Stenosis
Outcomes • 2 early deaths • 1 premature newborn with severe HMD • 1 post-op coarctation repair, 13 days post-BAV • 2 late deaths • Shone complex, COA repair, BMV, severe GER with aspiration pneumonia, PHT, sepsis • Borderline LV size, EFE, repeat BAVs, Ross/Konno (10 mo.), post-op PHT, RV failure
Outcome • Overall mortality rate: 8.8 % • Excluding coarctation repair, incidence of future intervention: 42% • Most common early intervention: repeat BAV • Most common late intervention: Ross procedure
Late clinical & echo findings • Early and mid-term follow-up available for 36/41 survivors 2.21 (.07 - 7.08) years • All survivors in good clinical condition • Peak instantaneous gradient: 29.5 + 19.5 torr • Mean gradient: 16 + 12 torr • AI grade: 0-1+ 28 2+ 7 3+ 1
Norwood/DKS after BAV • 2 patients referred • BDG in both, awaiting Fontan • LV volume: 25 ml/m2, 17 ml/m2 • Recoarctation in Norwood: BAA
Risk Factors for Reintervention • Repeat BAV: Initial gradient > 60 (odds ratio = 4.8) Age < 1 week (odds ratio = 3.4) • Ross: AI = 2+ (p = .02, odds ratio = 4.0)
Risk Factors for Norwood/DKS or Late Death • Coarctation (p = .03, odds ratio = 14.6) • EFE (p < .001, odds ratio = 38) • Small LV (3/4 LV Vol. Z score = -1.95) • LV morphology - not “apex forming” • Presence of severe MS (1 patient)
Conclusions • BAV successful in newborns even in the presence of coarctation • Reintervention is common • Repeat BAV successful for recurrent AS • Initial BAV does not preclude conversion to Norwood/DKS • Severe MS or persistent PHT with small LV preclude successful biventricular scheme
Conclusions • Ross procedure can be preformed safely beyond infancy allowing implantation of a larger PA allograft that should extend the time period before allograft replacement is needed.
How-to do BAV in newborn • Newborn female • Turner syndrome • 3.1 kg • Severe AS • Vmax = 4.8 m/sec • Mod. LVH • PFO present • Decision to proceed with BAV • Heparin given
LV angiography 8 mm annulus (LAO projection), 47 torr peak-to-peak gradient, mod. LVH
Aortic angiography No aortic insufficiency, normal coronary artery origins, hypoplastic transverse aorta
BAV .018 wire positioned in LV apex, 7 mm Nu MED Tyshak II balloon, hand inflation
Post-BAV Assessment Peak gradient = 5 torr, LVs = 98 -> 64 torr, mild AI, no injury to annulus, mitral valve, ascending aorta or coronary arteries