Download
1 / 53
530 likes | 707 Views
Cell Transplantation for the failing myocardium: A UK perspective Tony Gershlick U.H. Leicester BCIS meeting Bristol Sept 2005. Heart failure -strategies-. Medical treatment. Biventricular pacing Surgical cardiomyoplasty Left ventricular assist device Artificial hearts

E N D
Cell Transplantation for the failing myocardium: A UK perspective Tony Gershlick U.H. Leicester BCIS meeting Bristol Sept 2005
Heart failure -strategies- Medical treatment • Biventricular pacing • Surgical cardiomyoplasty • Left ventricular assist device • Artificial hearts • Heart transplantation • Cell transplantation ? • Therapy for AMI – • Lysis v PPC • Impact of time/treatment • 1 million UK heart failure • 5% all admissions • 1-2% health budget
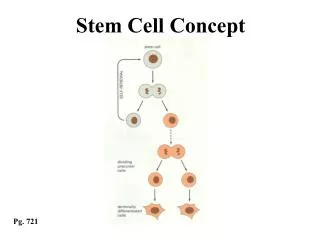
Stem cells for myocardial dysfunction Questions that (should) concern us in the UK Question 1 Is the science sound ?
Endothelial progenitor cells Intra myocardial primitive satellite cells Primative BM stem cells Skeletal muscle satellite cells
Transplanted adult bone marrow cells repair myocardial infarcts in mice.Orlic D, Kajstura J, Chimenti S, Bodine DM, Leri A, Anversa P.The left coronary artery was ligated and 5 hours later Lin- c-kit+bone marrow cells obtained from transgenicmalemice expressing enhanced green fluorescent protein - injected into the healthy myocardium adjacent to the site of the infarct. • 9 days the damaged hearts were examined for regenerating myocardium. • A band of new myocardium was observed in 12 surviving mice. • The developing myocytes were small and resembled fetal and neonatal myocytes. • - positive for EGFP, Y chromosome, and several myocyte-specific proteins including cardiac myosin, and the transcription factors GATA-4, MEF2, and Csx/Nkx2.5. • The cells were also positive for connexin 43, a gap junction/intercalated disc component Bone marrow transplantation –plenty of pre-clinical data Primative BM stem cells
Primitive cardiomyogenic cells from bone marrow Clin Invest, March 1999, Volume 103, Number 5, 697-70 Shinji Makino1, ball-like or stick-like appearance Fibroblast like spontaneously beating 5-azacytidine 2/52 beating cells were connected and formed myotube-like structures form myotube-like structures
Peripheral blood mononuclear cells Endothelial progenitor cells 1. Heamopoietic markers CD 34 + CD 133 + 2. Endothelial markers EGF -2
A EPC transdifferentiate in-vitro into cardiomyocytes Intracellular gap junctional coupling between rat cardiomyocytes and human EPCs was demonstrated Badorff et al, Circulation 2003;107:1024-1032 B Human EPCs transplanted into rat infarct model day 7 Therapeutic Potential of Ex Vivo Expanded Endothelial Progenitor Cells for Myocardial Ischemia Atsuhiko Kawamoto Circulation. 2001;103:634 Angiogenic potential / neo-vascularisation
Myoblasts are satellite cells and exist in a quiescent state. They have built in resistance to ischemia
Myotubes with prominent normal Z bands in myofilaments and peripheral multiple nuclei in myotubes grafted skeletal myotubes replacing scar fibrosis Myoblast grafts can survive and show a switch to slow-twitchfibres. Do not become myocytes Hagege et al, Lancet 2003;361:491-92
Science :Good In-vitro, ex-vivo, animal data for BMC, EPC , Myoblast all have potential Which will be clinically applicable ?
What is actually happening ? Autologous bone marrow cells Circulating progenitor cells Skeletal myoblasts Manipulation of in-vivo cells Ischaemia (AMI) Chronic Heart Failure
Questions that (should) concern us in the UK • Is the basic science sound • Are the trials of sufficient quality to provide the answers to the questions being asked ? • Are the trials relevant to our current practice ?
MNC MNC v CPC MNC MNC
Circulation, December 10, 2002 • 20 patients with reperfused acute myocardial infarction • received bone marrow-derived stem cells (n=9) CPC (n=11)250mls • Non-randomized matched reference group • Trial end-point: LVEF assessed by Echo and PET-Scan @ • 4 months follow-up and at one year
TOPCARE-AMI LVEF 51.3% 59.5% 8.2% Would they have got better 2 nd to PCI anyway? Improved myocardial viability in the stem cells group
The Lancet, July 10, 2004 • First randomized clinical trial • after successful percutaneous • coronary intervention (PCI): • 30 patients control group, • 30 patients bone-marrow cell group • Primary endpoint: global left-ventricular ejection fraction • (LVEF) change from baseline to 6 months’ follow-up, • determined by cardiac MRI
BOOST Mean in-stent restenosis in the infarct-related artery, expressed as a percentage of luminal diameter, was 32% (SD 20) in the control group and 33% (23) in the bone-marrow-cell group (p=0·88). Four patients from the control group and seven from the bone-marrow-cell group presented with an in-stent restenosis of at least 50% (p=0·28).
Problems with the acute ischaemic trials Unanswered clinical trial questions Trials don’t tell us which cells Variable numbers of cells transplanted – both CPC and BMC 3-5% : (Stem cell selection~ 200 mls BM) Retention 3% Benefit did not correlate with absolute numbers of CD 34 cells Unselected and selected cell populations not compared No dose ranging studies Timing? Early environment cyto-toxic 3- 7 days ? longer Engraftment
All P PCI Small number subjects -pilot studies (Mortality/ morbidity end point (1000 s patients) No adequate controls (Bone marrow acquisition?, coronary manipulation ?) EF increases small Mode of Delivery Who is likely to benefit ? • Problems with the acute clinical trials X No clear messages re type cells, nos. and delivery “REPAIR AMI” AHA
Appropriate trials ? • Who most likely to benefit ? • Cell type ? • Which of these questions can be answered ? • What is the UK involvement • Can we add to the Clinical science?
UK Centres Involved in Stem Cell Therapy UHL/ St Barts/ The London Anthony Mather Martin Rothman John Martin Eric Alton Kings College Hospital Jonathan HillAJ Shah St Marys/ Brompton Nic Peters Philip Poole-wilson UH Leicester Jan Kovac Manual Galinanes Nilesh Samani Tony Gershlick
Failure of thrombolysis Successful R-PCI Echo d 3 EF < 45% Baseline MRI SC or Heparinised plasma d 4-5 P EP 4 mo MRI Poor LV Setting lysis + RESCUE-PCI Late phase
Clinical ‘stem cell’ trials - Barts and the London NHS Trust/UCLH • Randomised control trials using autologous bone marrow derived mononuclear cells in patients with: • Heart failure 2o IHD - commenced 8/05 - 300 patients • Dilated cardiomyopathy - recruiting - 200 patients • AMI tx with primary angioplasty - funding sort - 200 patients • PIs: A Mathur, M Rothman, J Martin
Which of these questions can be answered, What is the UK involvement • Appropriate trials ? • Who most likely to benefit ? • Cell type ?
Muscular Biopsy • Myoblast cells liberated through Enzymatic Digestion intercellular matrices
Alternative Therapies For the Treatmentof Ischemic Cardiomyopathy LVEF/NYHA IMPROVEMENT AT SIX MONTHS LVEF NYHA % Change Journal of the American College of Cardiology, Vol. 42, No. 12, 2003, Smits, Serruys et al. Patient Study. Study sponsored by Bioheart, Inc. 3 month, P=0.009, n=5; 6 month, P= 0.23, n=5.
Bioheart Percutaneously Delivered Myoblasts EU Phase II Trial (SEISMIC™) ICD EF > 20% < 40 % 8 European Centres 3 UK :Glenfield, (AHG,JK) Leicester St Marys (Nic Peters) Royal Brompton (Philip Poole-Wilson - 6) : Standard medical therapy Screening: 46 ICD patients Baseline Evaluation Visit 1 (Week Randomization ICD patients: 30 MyoCell ™ , 16 Treatment Arm Control Arm ( Myocell 150 - 800 x 10 ) (Standard Medical Therapy) TM 6 16 ICD patients 30 ICD patients - Enrollment Began June 2005.
SEISMIC Safety Endpoints Primary: • Defined Serious Adverse Events (SAEs) Secondary: • Routine Clinical laboratory test results • Holter monitoring, 12-lead ECG data • Overall patient survival • Assessment of the safety of the use of the MyoCath™, by Adverse Event assessment
SEISMIC Efficacy Endpoints Primary: • Change in LVEF at 3 and 6 months by MUGA compared with baseline Secondary: • QOL Assessments (6-min. walk, NYHA class) • Hospitalization, readmissions or the need for medical treatment outside of hospitalizations • Echocardiography (global contractility, wall thickness and coronary perfusion improvements)
British Collaborative on Stem Cell Research and the Heart Objective: To form a collaborative group of basic scientists and clinicians involved in research in stem cells and the heart, in order to perform joint research. • Four meetings held in UCL, average attendance 50 people. • Three groups formed: stem cells and vectors animal models clinical trials
British Collaborative on Stem Cell Research and the Heart • A “writing group” has met to define what clinical and basic research needs to be done. Joint grants will be applied for. A document will be circulated shortly. • The clinical group will peer review protocols with an emphasis on safety and necessity of studies. • The group has a close connection to the European Society of Cardiology Task Force on Stem Cells and the Heart
General Summary and Conclusions • Too soon to draw any conclusions • Studies small, all PPCI, ? Safety concerns (restenosis) • Promising
Bone-marrow stem cell Post AMI patient • Advantages • Pluripotent stem cells can develop into cardiomyocytes • Easy to isolate and grow well in culture • Neovascularization can also occur at the site of the scar • Can improve myocardial function • Limitations • New program of cell differentiation program is required • Efficiency of differentiation into adult cardiomyocytes may be limited • Some studies difficult to replicate • Small trials • LV improves anyway • UK PPCI makes applicability difficult Trials to date uncontrolled small numbers un-blinded
Skeletal myoblasts Chronic HF AMI patient • Limitations • Likely do not develop new cardiomyocytes in vivo • Electrical coupling to surrounding myocardial cells is probable but not definite • Long-term stability of differentiated phenotype is unknown • Arrhythmic potential • Advantages • Cells proliferate in vitro • Ischemia resistant • Transplanted cells can differentiate into slow-twitch myocytes, enabling cellular cardiomyoplasty • Reduce dilatation and improve cardiac function • Can use adult cells
Transplantation of progenitor Cells AMI patients • Intracoronary infusions are safe and feasible • Increase in global LVEF • Improvement in wall motion abnormalities • Reduction in LVESV • Complete normalization of CFR(< so in BMC) • Increases in myocardial viability May need cytokines like G–CSF and this may be a problem
Stem Cell Tx appears to “work” Issues and questions 1 How long will the transplanted cells survive? Can they be safely delivered PCI/endocardially Are they able to integrate? Modified ? Do they have the ability to differentiate? Will the cell transplant influence LV function? Can we augment/enhance grafting, proliferation and function of stem cell implants? Is it safe ?
Issues and questions 2 • How many cells do we need to transplant? • Which is the best way for delivery? • Should the donor cell chosen depend on the cause of heart failure/ ventricular dysfunction ? • Which is the optimal time for cell transplantation? • What trials are needed to provide definitive answers ? • UK is involved, central organisation, • Funding, Regulatory bodies (MHRA,COREC) collaboration, need for multi discipline are all challenges
Cell transplantation is an exciting development Many questions NEED SUFFICIENTLY POWERED RANDOMISED CONTROLLED TRIALS Something (UK) interventional cardiologists need to be involved in Watch this space - new era for interventional cardiology “EPC > Bone marrow > myoblasts “ • True quantity of effect • That it is the SCT that is having any effect • Safe