Download
1 / 48
480 likes | 624 Views
Human Immunodeficiency Virus in Women. Lori E. Kamemoto, MD, MPH Department of Obstetrics, Gynecology and Women’s Health University of Hawaii. HIV in Women. 1. Epidemiology 2. Sexual Transmission and post- exposure prophylaxis 3. Contraception 4. Gynecologic problems

E N D
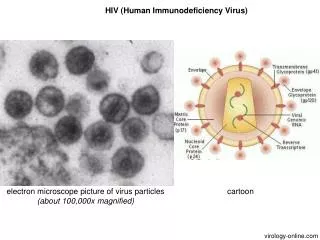
Human Immunodeficiency Virus in Women Lori E. Kamemoto, MD, MPH Department of Obstetrics, Gynecology and Women’s Health University of Hawaii
HIV in Women 1. Epidemiology 2. Sexual Transmission and post- exposure prophylaxis 3. Contraception 4. Gynecologic problems HPV disease
HIV in Women USA: 24% of all AIDS cases are women (1999) Hawaii: 8% of all AIDS cases are women (1994-9) Worldwide: more than 40% of all adult HIV infections are women (75% of all new infections)
AIDS in Women, U.S. Estimated 1,080 50+ AIDS cases in 1996 CDC, 1998
Most Common AIDS-indicator Diseases in Women *some with more than one diagnosis, CDC, 1992
Sex Differences in HIV • Women have a lower viral load than men • Time to development of AIDS was similar in men and women • Women with the same viral load as men had a higher risk of AIDS (OR = 1.6, 95% CI 1.1-2.32) • Suggests that viral load recommendations for antiretrovirals may need to be revised downwards for women Farzadegan, etal. Lancet, November 7, 1998
HIV Infection in WomenSexual Transmission Homosexual Men Men infected by Blood products Male IVDU Bisexual Men Infected Sperm Donors WOMEN Homosexual Women
HIV Prevention Key Strategies • Prevent HIV • Determine HIV status • Treat HIV as early as possible
Barriersto HIV Testing in Women • No prenatal care (15% of HIV+ have no prenatal care) • Heavy clinic load • When health care providers strongly recommend testing (routine prenatal test), patient 3 times as likely to get tested • Patient afraid of testing Ickovics, 1999
Worldwide, the most common mode of HIV transmission isSEXUAL TRANSMISSION
Sexual Transmission of HIV • Probability of HIV transmission with vaginal intercourse: 0.1% • Women about twice as susceptible to heterosexual transmission of HIV than men • Probability of HIV transmission with anal intercourse: 0.5-3% Lurie, JAMA, 1998
HIV in the Female Genital Tract • HIV detected in cervicovaginal secretions and cervical tissue • Increased rate of cervical HIV shedding with cervical ectopy, cervicitis, pregnancy, oral contraceptives and increased serum viral load • Decreased genital tract HIV with anti-retrovirals Critchlow CW, OBGyn Survey 1997
Chlamydia and HIV Transmission • Chlamydia may increase susceptibility to HIV • Prostitutes with Chlamydia cervicitis had a 3 times higher risk for HIV seroconversion • Chlamydia causes mucosal friability, bleeding and an inflammatory response Laga M. Sixth Int’l Conf on AIDS, 1990
Male Circumcision and HIV infection Risk • Thirty studies reviewed • 22 studies reported a significant association between circumcision and HIV + status (RR 1.5 - 8.4) (4 studies with a trend towards association and 4 studies with no association) Moses. STD 1994
DepoProvera and HIV Transmission • 1996 - SIV contracted by 14/18 monkeys on progesterone implants • 1/10 not on implants implants HIV infected • Hypothesis: thinning of the monkeys’ vaginal epithelium increased risk of transmission • Martin (Kenya) - women on DepoProvera had an increased risk of HIV infection (OR 2.2, 95% CI 1.3-3.1) • Other human studies show no increased risk Martin HL. J of Inf Dis, October 1998
Vaginal Microbicides • Need to develop methods that a woman can control to help prevent sexual transmission of HIV • Various vaginal microbicides are currently being studied
Needlestick Injuriesto Health Care Workers • HIV -22 published studies -0.25% (1 in 400) risk of seroconversion from needlestick -0.09% (1 in 1,000) risk of seroconversion from mucous membrane exposure -chemoprophylaxis is the standard of care • Hepatitis B: 5-60% chance of infection
HIV Postexposure Prophylaxis • NO randomized studies exist • Biologically plausible • Scientific evidence animal models ARV prophylaxis in pregnancy studies support PEP
HIV Postexposure Prophylaxis after Sexual Contact • Probability of HIV transmission with vaginal intercourse 0.05-0.15% anal intercourse 0.8-3.2% • If the partner’s HIV status is known, recommend prophylaxis • If the partner’s HIV status is unknown, decision based on type of exposure and likelihood of HIV in the partner • Several probable cases of HIV transmission from rape reported Katz. JAMA 1997
Postexposure Prophylaxis afterNon-occupational HIV Exposure “The probability of HIV transmission by certain sexual or injection drug exposures is of the same order of magnitude as percutaneous occupational exposures for which the CDC recommends PEP.” “In such cases, if the exposure is sporadic, it seems appropriate to extrapolate from the data on occupational PEP and recommend prophylaxis” JAMA 1998
Assessing Risk of HIV Transmission after Non-occupational Exposure Probability of HIV infection depends on: • frequency of exposure • probability that the source is HIV + • probability of infection if the source is HIV +
HIV infected WomenSexual Behaviors • Heterosexual activity in the last 6 months HIV positive 65% HIV negative 76% • Always use a condom with vaginal intercourse HIV positive 63% HIV negative 28% Wilson TE. AIDS, April 1999 (WIHS)
Emergency Contraception • Plan B: levonorgestrol • Must be taken within 72 hours of intercourse • 89% effective in preventing pregnancy • No studies on HIV infected women
Birth Control Pills and AntiretroviralsHIV + Women • Efavirenz increases estradiol levels (AUC 37%) • Nevirapine decreases estradiol levels (AUC 19%) • Ritonavir decreases estradiol levels (AUC 41%) • Nelfinavir decreases estradiol levels (AUC 47%) • Birth control pills may not be effective with certain antiretrovirals
DepoProveraHIV+ Women • No data on progesterone levels and antiretrovirals • DepoProvera and Antiretrovirals study currently in enrollment • Many HIV infected women choose this method of birth control
IUDsHIV+ Women • Theoretical concern regarding increased risk of uterine infection and PID with immuno- compromised patients • African study seemed to validate safety in their population, however these patients were not followed long term
Gynecologic Problems and HIV • Severe, recurrent yeast vulvovaginitis Rhoads: 24% of HIV+ women had chronic candidiasis • Severe, recurrent genital Herpes • Syphilis may follow an accelerated course • Human Papilloma Virus infections occur more frequently and are more severe • Trichomonas infections are more severe • PID possibly more severe
Longitudinal Study of HPV in HIV infected Women • Prevalence of HPV at baseline HIV + 73%, HIV neg 43% • Prevalence of high risk oncogenic HPV at baseline HIV + 32.5%, HIV neg 17% • HIV + women with lower CD4 counts had a higher prevalence of HPV
Abnormal pap smears in HIV infected Women *African studies
Innoculation Incubation period: HPV DNA establishes itself Active lesion growth 3-6 months 9 months from the time of the first lesion: equilibrium between lesion growth and host immune response sustained remission or continued active lesions Stages of HPV Infection
A Shared Etiology for all Anogenital Cancers? • Cancers associated with HPV infection • Cervical • Vulvar, vaginal • Anal • Penile • Common risk factors • Smoking • STDs, sexual activity • Factors that may not support shared etiology • Cervical cancer incidence peaks at age 40-50; other anogenital cancers continue to increase with age • Penile cancer does not seem to be increasing, slight increase in vulvar cancer, anal cancer increasing
AnoGenital Dysplasia and HIVInteraction between HIV and HPV • HPV infection restricted to the epithelium and HIV infection primarily in the stromal cells/T-cells/Langerhans cells (1) and (2) • Pathogenesis theories • decreased cell mediated immunity to HPV • HIV and HPV may co-infect the same epithelial cells (3) • HIV infected cells may secrete factors that up-regulate HPV infection Palefsky J, Monogr Natl Cancer Inst, 1998
Anogenital Disease and HIVImmune ResponseModel • HPV infection acquired early with onset of sexual activity, followed by HIV • Early HIV infection: immunity relatively intact and no anogenital lesions • Late HIV infection: increased HPV levels and anogenital lesions Palefsky J, Monogr Natl Cancer Inst, 1998
Anogenital Disease and HIVImmune Response Model • Restoration of immune response with HAART regression of HSIL • If HAART leads to prolonged life, but does not fully restore immunity to HPVcancer Palefsky J, Monogr Natl Cancer Inst, 1998
23 year old G1 HIV+ woman who is 37 weeks pregnant and on combination ARVs On pelvic examination, she is noted to have multiple condylomatous growths on the vulva CD4=300 and viral load=8,000 Gyn Case Presentation
Vulvar biopsy reveals condyloma Cesarean section is performed You ask her to follow-up in 3-4 months and on this visit, most of her condyloma has now disappeared She is still taking her ARVs A pap smear is done and you ask her to follow-up in another 3-4 months Gyn Case Presentation
Her pap smear revealed ASCUS She complains of vulvar itching Flat hyperplastic lesions are noted on the vulva She was recently discharged from the hospital (PCP) Gyn Case Presentation
Cervical and vaginal lesions are also noted on colposcopy and biopsies are done Gyn Case Presentation
Biopsies reveal: 1. Cervical severe dysplasia, cannot rule out cancer 2. Vaginal biopsies reveal VaIN 1 3. Vulvar biopsies reveal VIN 2-3 Procedures: 1. Cervical conization 2. Laser vulva You ask her to follow-up in another 4-6 months Gyn Case Presentation
Another pap smear and colposcopy is done You note that she still has a few residual vulvar raised lesions A repeat pap smear and colposcopy is done HPV disease waxes and wanes depending on patient immune status-HIV+ women need to be followed closely Gyn Case Presentation