Download
1 / 58
580 likes | 916 Views
MU: The Regulatory Context. . . . . . ARRA specifies three requirements for

E N D
1. Regulatory context
Objectives, stages and final rule
Eligibility, incentive payments
Regulatory context
Objectives, stages and final rule
Eligibility, incentive payments
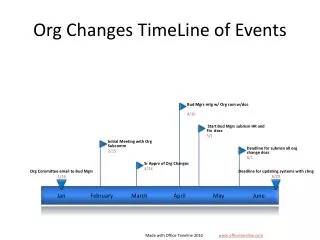
4. Meaningful Use: Timeline of Events 2009
February 17, 2009 � Obama signs ARRA. HITECH (Health IT for Economic and Clinical Health) provisions include meaningful use (MU).
January 13, 2009 - Draft rule on MU incentive payments
2010
March, 2010 - NACHC & CHCANYS submit official comments (over 2000 comments)
February 23 & March 29, 2010 - New York State Medicaid solicits testimony from CHCANYS
July 13, 2010 � Final Rule released
2011
Medicaid Incentive Program:
Certification process and timeline to be published by NY State Medicaid
Medicare Incentive Program:
January, 2011 - begin the 90-day process of using a certified record per meaningful use requirements
April, 2011 � Attestation for Meaningful Use
May 2011 � CMS Payments begin
6. Sandy � is working on Payment Mechanism ok?Sandy � is working on Payment Mechanism ok?
18. Adopt, Implement, Upgrade (AIU)
In their first year of participation in the Medicaid incentive payment program, EPs may qualify for an incentive payment by demonstrating any of the following: �
that they have adopted (acquired),
implemented (installed or commenced utilization, e.g. staff training, data entry, redesign of provider workflows, or establishing data exchange agreements), or
upgraded (upgrade to a certified version or expanded functionality, e.g. CDSS, e-prescribing, or other features that facilitate meaningful use)
This casts a wide net
Final definition and documentation requirements to be announced by NYS Medicaid
21. Medical Home Tenets Adopted by AAFP, ACP, AAP, AOA:
Personal physician
Physician directed medical practice
Whole person orientation
Care is coordinated and/or integrated
Quality and safety
Enhanced access
Payment
www.medicalhomeinfo.org/Joint%20Statement.pdf. Accessed May 9, 2008. A. Personal physician�each patient has an ongoing
relationship with a personal physician trained to provide
first contact, continuous and comprehensive care.
B. Physician directed medical practice�
the personal physician leads a team of individuals at
the practice level who collectively take responsibility
for the ongoing care of patients.
C. Whole person orientation�the personal
physician is responsible for providing for all the patient�s
health care needs or taking responsibility for appropriately
arranging care with other qualified professionals.
This includes care for all stages of life; acute care; chronic
care; preventive services; and end of life care.
D. Care is coordinated and/or integrated across
all elements of the complex health care system (e.g.,
subspecialty care, hospitals, home health agencies, nursing
homes) and the patient�s community (e.g., family, public
and private community-based services). Care is facilitated
by registries, information technology, health information
exchange and other means to assure that patients get the
indicated care when and where they need and want it in
a culturally and linguistically appropriate manner.
E. Quality and safety are hallmarks of the
medical home:
� Practices advocate for their patients to support the
attainment of optimal, patient-centered outcomes
that are defined by a care planning process driven
by a compassionate, robust partnership between
physicians, patients, and the patient�s family.
� Evidence-based medicine and clinical decision support
tools guide decision making.
F. Enhanced access to care is available through
systems such as open scheduling, expanded hours and
new options for communication between patients,
their personal physician, and practice staff.
G. Payment appropriately recognizes the added value
provided to patients who have a Patient-Centered
Medical Home. The payment structure should be based
on the following framework:
� It should reflect the value of physician and non physician
staff patient-centered care management
work that falls outside of the face-to-face visit.
� It should pay for services associated with coordination
of care both within a given practice and between
consultants, ancillary providers, and community
resources.
� It shouldA. Personal physician�each patient has an ongoing
relationship with a personal physician trained to provide
first contact, continuous and comprehensive care.
B. Physician directed medical practice�
the personal physician leads a team of individuals at
the practice level who collectively take responsibility
for the ongoing care of patients.
C. Whole person orientation�the personal
physician is responsible for providing for all the patient�s
health care needs or taking responsibility for appropriately
arranging care with other qualified professionals.
This includes care for all stages of life; acute care; chronic
care; preventive services; and end of life care.
D. Care is coordinated and/or integrated across
all elements of the complex health care system (e.g.,
subspecialty care, hospitals, home health agencies, nursing
homes) and the patient�s community (e.g., family, public
and private community-based services). Care is facilitated
by registries, information technology, health information
exchange and other means to assure that patients get the
indicated care when and where they need and want it in
a culturally and linguistically appropriate manner.
E. Quality and safety are hallmarks of the
medical home:
� Practices advocate for their patients to support the
attainment of optimal, patient-centered outcomes
that are defined by a care planning process driven
by a compassionate, robust partnership between
physicians, patients, and the patient�s family.
� Evidence-based medicine and clinical decision support
tools guide decision making.
F. Enhanced access to care is available through
systems such as open scheduling, expanded hours and
new options for communication between patients,
their personal physician, and practice staff.
G. Payment appropriately recognizes the added value
provided to patients who have a Patient-Centered
Medical Home. The payment structure should be based
on the following framework:
� It should reflect the value of physician and non physician
staff patient-centered care management
work that falls outside of the face-to-face visit.
� It should pay for services associated with coordination
of care both within a given practice and between
consultants, ancillary providers, and community
resources.
� It should
22. National Committee for Quality Assurance (NCQA) and the PCMH NCQA developed a set of standards and a 3-tiered recognition process to assess the extent to which health care organizations are functioning as medical home
Obtaining recognition requires completing an application and providing adequate documentation to show evidence that specific processes and policies are in place
Recognition is offered at three levels:
Level 1
Level 2
Level 3
23. NCQA Score Requirements The NCQA scoring guidelines for the PCMH has 3 levels of achievement
There are 10 Must-Pass elements, of which a practice must pass at a 50% or greater score.
A practice must pass 5 of the 10 must pass elements for Level 1 recognition, and 10 of the 10 elements for Level 2 or 3 recognition
The NCQA scoring guidelines for the PCMH has 3 levels of achievement
There are 10 Must-Pass elements, of which a practice must pass at a 50% or greater score.
A practice must pass 5 of the 10 must pass elements for Level 1 recognition, and 10 of the 10 elements for Level 2 or 3 recognition
24. Benefits of PCMH
25. NY State PCMH Incentive Payment For claims coded with E&M and/or Preventive Medicine codes
For fee-for-service claims
$5.50 for Level 1
$11.25 for Level 2
$16.75 for Level 3
For Medicaid Managed Care & Family Health Plus claims
Plans receive $2/$4/$6 PMPM for Levels 1/2/3
Payments must go to recognized practices; cannot be retained by Plans or rolled over to subsequent year
Plans will provide details on payout method
Payments for Level 1 will end after December 2012 to promote practices obtaining Levels 2 & 3 recognition
26. The NCQA PPC-PCMH Survey NCQA framework can be used as a framework for a systematic approach to ensuring we are actually doing what we intend to do.
NCQA framework can be used as a framework for a systematic approach to ensuring we are actually doing what we intend to do.
27. Standards Standards are definitive statements about acceptable performance or results
Each Standard
includes a statement of an attribute or expectation
has a designated number of points which is the sum of points from all elements assigned to the standard
Has a statement of intent that describes the purpose of the standard
Example: PPC1 (or Standard 1), Access and Communication [9 points]
Statement: The practice has standards for access to care and communication with patients and monitors its performance to meet the standards
Intent: The practice provides patients with access during & after regular business hours, and communicates with patients effectively
28. Elements There is at least one Element for each Standard
Each Element
has specific number of points
describes a specific component of performance that is individually evaluated and scored
Example: PPC 1A, Access & Communication Processes [4 points] & PPC 1B, Access & Communication Results [5 points]
PPC 1A: The practice establishes in writing standards for the following processes to support patient access
PPC 1B: The practice�s data show that it meets access & communication standards in PPC 1A
29. Must Pass Elements These are 10 of the 30 Elements that a practice must pass at a 50% or greater score in order to achieve any level of recognition (5 for Level 1; 10 for Level 2 or 3)
They are considered to be the fundamental building blocks for a medical home that any practice must be able to demonstrate to be a medical home
31. Peter :
Welcome
Expectation:
Not scholarly
Developing a conversation about what people are struggling with and what needs they have
Focsed on NYS
Trying to engage in a conversations that produces an understanding of the needs in the community
Housekeeping
Introduce the Speakers/The Panel�.who you�ll hear from 2day
Peter :
Welcome
Expectation:
Not scholarly
Developing a conversation about what people are struggling with and what needs they have
Focsed on NYS
Trying to engage in a conversations that produces an understanding of the needs in the community
Housekeeping
Introduce the Speakers/The Panel�.who you�ll hear from 2day
32. Criteria for Achieving Meaningful Use & PCMH Meaningful Use (MU)
Improve quality, efficiency and reduce health disparities
Engage patients & families
Improve care coordination
Improve population & public health
Ensure privacy & security
PCMH
Access & communication
Patient tracking & registry
Care management
Patient self-management
Electronic prescribing
Test tracking
Referral tracking
Performance reporting & improvement
Advanced electronic communications
Lisa PerryLisa Perry
33. Is this a good place to quantify the overlap? Your intro slide does ask �How much do they have in common?�
I don�t remember the figures, but they were interesting and demonstrate how much overlap there is.Is this a good place to quantify the overlap? Your intro slide does ask �How much do they have in common?�
I don�t remember the figures, but they were interesting and demonstrate how much overlap there is.
34. I don�t understand �Cut of PCMH Factors that could apply HIT�
Are you saying these are the PCMH Factors that either require or will be significantly easier with HIT?
An alternative subtitle could be �PCMH Factors that require or benefit from use of HIT�I don�t understand �Cut of PCMH Factors that could apply HIT�
Are you saying these are the PCMH Factors that either require or will be significantly easier with HIT?
An alternative subtitle could be �PCMH Factors that require or benefit from use of HIT�
37. PCMH Application Checklist Obtain free copy of NCQA PPC-PCMH Standards & Guidelines available at http://www.ncqa.org/tabid/629/Default.aspx#pcmh
Purchase $80 NCQA PPC-PCMH Survey Tool available at http://www.ncqa.org/tabid/629/Default.aspx#pcmh
Determine survey approach if part of multi-site network (multi-site or standard survey)
38. PCMH Application Checklist Complete NCQA PPC-PCMH Application Documents
Compile PPC-PCMH submission
Identify three clinically important conditions
Develop system for labeling and organizing documentation required for submission (nomenclature should clearly identify relevant factor(s); if using multi-site option, should clearly indicate relevant site(s))
Compile documentation required for submission
Identify 36 patients to include in chart review and conduct chart review for relevant elements (2C, 2D, 3D, 4B) (refer to NCQA�s Record Review Workbook for information regarding the methodology for selecting your sample and tool to use to conduct chart review)
Upload documentation and complete on-line survey (including notes to reviewer)
Application documents must be completed and returned to NCQA prior to uploading documentation and completing submission; should be completed at least 2-4 weeks prior to anticipated submission date to avoid delays to timeline.
Agreement (includes Attestation, Data Release, NCQA Agreement and HIPAA Business Associate Agreement)
Practice Background Information Worksheet
Application, including submission date
Multi-Site Group Survey Assessment Questionnaire (if interested in using multi-site survey option)
Determine fee (refer to NCQA PPC-PCMH Fee Schedule available at http://www.ncqa.org/tabid/631/Default.aspx); NCQA accepts checks and credit cards
Application documents must be completed and returned to NCQA prior to uploading documentation and completing submission; should be completed at least 2-4 weeks prior to anticipated submission date to avoid delays to timeline.
Agreement (includes Attestation, Data Release, NCQA Agreement and HIPAA Business Associate Agreement)
Practice Background Information Worksheet
Application, including submission date
Multi-Site Group Survey Assessment Questionnaire (if interested in using multi-site survey option)
Determine fee (refer to NCQA PPC-PCMH Fee Schedule available at http://www.ncqa.org/tabid/631/Default.aspx); NCQA accepts checks and credit cards
40. MU Checklist: 2010 & 2011 Prepare for upgrade to certified version of your EHR
Contact vendor to learn upgrade process and requirements (may include upgrade of related software and/or hardware)
Schedule your upgrade
Prepare for upgrade
Develop a team
Conduct communications campaign with Board, patients & staff
Calculate your % �needy individuals� for CY 2010 to determine that your health center meets the 30% threshold
Identify your Eligible Professionals
Register them for 2011 MU incentives & assignment
Stay tuned for further instructions from NY State Medicaid
Attest for each provider that you have satisfied requirements of �Adopt, Implement, or Upgrade�
41. MU Checklist: Now - 2012 Conduct detailed self-assessment & gap analysis for Stage 1 MU
Develop work plan
Begin system configuration, workflow revision, training, report development & other activity required to achieve each MU objective
Compile documentation of compliance with each MU Objective for 90-days in 2012
Attest for each provider
42. Regional Extension Centers (RECs) have been funded to provide technical assistance in achieving MU
CHCANYS is an extension agent of the NYeC REC, serving all FQHCs in New York State except those in New York City
New York City FQHCs are served by REACH, the NYC DOHMH REC
Please contact us if you are interested in more information:
Sandy Worden sworden@chcanys.org
Lisa Perry lperry@chcanys.org
44. Additional Resources: Educational Materials For Patients
Brochure in 14 languages
Video by Emmi Solutions to explain the PCMH concept for patients is available at: http://www.emmisolutions.com/medicalhome/transformed/
For Providers
Educational brochure
Three part series of presentations on PCMH can be viewed and downloaded at: http://www.acponline.org/running_practice/pcmh/ �
See the right hand column: �What is the PCMH?� and �Common Questions About the PCMH.�
Provider PowerPoint, above brochures and more available at: http://www.ehealth4ny.org/resources.html
FAQs on Meaningful Use and additional resources available at http://www.nyecrec.org/index.php/education-a-resources
56. Standards & Certification: Timeline of Events 2010
January 13, 2010 - Official publication in Federal Register of Initial Set of Standards, Implementation Specifications & Certification Criteria for Electronic Health Record Technology; effective 30 days after publication
60-day comment period
June 24, 2010 � Official publication in Federal Register of Final Rule re: temporary certification program
July 13, 2010 � Release of Final Rule on Standards & Certification Criteria
August � September, 2010 � First Authorized Testing & Certification Bodies to be named
Fall, 2010 � Anticipated time for certified products to be available on market
57. Key Definitions Standard - a technical, functional, or performance-based rule, condition, requirement, or specification that stipulates instructions, fields, codes, data, materials, characteristics, or actions. (e.g. HIPAA codes, HL7, CCD)
Implementation Specification - specific requirements or instructions for putting a standard into operation
Certification Criteria �
to establish that health IT meets applicable standards and implementation specifications adopted by the Secretary;
to test and certify that health IT includes required capabilities.
58. Standards, Implementation & Certification: Relationship to MU Relationship to Meaningful Use:
The HITECH Act fundamentally ties the standards, implementation specifications, and certification criteria adopted in this IFR to the incentives available under the Medicare and Medicaid EHR Incentive Programs by requiring the meaningful use of Certified EHR Technology.
Certification criteria described in the IFR:
establish the capabilities and standards that certified EHR technology will need, at a minimum, to support the achievement of proposed meaningful use Stage 1 by EPs and hospitals.