Download
1 / 29
310 likes | 2.19k Views
Pulmonary Atelectasis. Presented by Kang, ting-jui. Introduction. General anesthesia is associated with impaired oxygenation pulmonary atelectasis was suspected as the major cause Decrease in lung compliance and the partial pressure of arterial oxygen (PaO2)

E N D
Pulmonary Atelectasis Presented by Kang, ting-jui
Introduction • General anesthesia is associated with impaired oxygenation pulmonary atelectasis was suspected as the major cause • Decrease in lung compliance and the partial pressure of arterial oxygen (PaO2) • Atelectasis occurs in the most dependent parts of the lung of 90% of patients who are anesthetized gas exchange abnormalities and reduced static compliance associated with acute lung injury perioperative morbidity
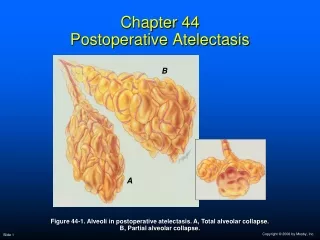
Physiologic causes of atelectasis • Mechanisms: • Compression of lung tissue • Absorption of alveolar air • Impairment of surfactant function
Compression atelectasis • Overall cephalad diaphragm displacement after anesthesia, the diaphragm is relaxed • Differential regional diaphragmatic changes • In an anesthetized patient breathing spontaneously the diaphragm moves the most in the lower, dependent portion • During paralysis and positive-pressure ventilation the passive diaphragm is displaced by the positive pressure preferentially in the upper, nondependent portion
Compression atelectasis • Shift of thoracic central vascular blood into the abdomen additional dependent pressure arising from the abdomen • Altered diaphragmatic dynamics phrenic nerve stimulation versusisovolumic conditions in anesthetized patients
Gas resorption • Resorption atelectasis occur by two mechanisms • After complete airway occlusion gas trapped gas uptake by the blood continues and gas inflow is prevented gas pocket collapses; increases with elevation of FI02 • Low ventilation relative to perfusion (low [VA/Q] ratio) have a low partial pressure of alveolar oxygen (PAO2) when FIO2 increased, PAO2 increases oxygen moves from alveolar to blood greatly lung unit progressively smaller
Surfactant impairment • Stabilizing function of surfactant may be depressed by anesthesia • Reduction in percent maximum lung volume was proportional to the concentration of both chloroform and halothane • Halothane anesthesia combination with high oxygen concentration, caused increased permeability of the alveolar– capillary barrier in rabbit lungs • Increased tidal volume cause release of surfactant
Type of anesthesia • Atelectasis develops with both intravenous and inhalational anesthesia, whether the patient is breathing spontaneously or is paralyzed and mechanically ventilated • Ketamine: not produce atelectasis when used alone • Regional anesthesia: depend on the type and extension of motor blockade • Reduces inspiratory capacity by up to 20%, and expiratory reserve volume approaches zero • Less extensive blockade closing capacity and FRC remain unchanged
Impact of time • The maximum decrease in FRC seems to occur within the first few minutes of general anesthesia • During anesthesia for surgical operations on the limb FRC is not influenced further by depth or duration of anesthesia • During abdominal or thoracic surgery, pulmonary gas exchange deteriorates progressively during the course of the operation unable to determine the independent impact of time on atelectasis as opposed to surgical manipulation
Effects of position • Changing from the upright to the supine position results in a decrease of 0.5L in FRC to 1.0L, even in the awake state • After anesthesia, FRC is reduced by a further 0.5L to 0.7L • Trendelenburg position resulting in further decrease in FRC • Lateral decubitus position usually slight increase in total lung FRC • Prone position may increase FRC slightly, although this may not decrease atelectasis
Effects of position • Distribution of ventilation is more uniform in anesthetized patients in the prone position; improves oxygenation in patients with ARDS • Atelectasis is more prominent after cardiac surgery with cardiopulmonary bypass; not related to increasing in pulmonary endothelial permeability • Lung recruitment strategy and PEEP improves oxygenation in patients after CPB • Intentionally inflate the patient’s lungs before coming off CPB and directly visualize equal expansion of the lungs
Inspired oxygen • High oxygen concentration has been associated with atelectasis formation • Increasing FIO2 at the end of surgery to 1.0 before extubation also causes additional atelectasis • During routine induction of general anesthesia, 80% oxygen caused minimal atelectasis, but the time margin before desaturation occurred was significantly shortened compared with that of 100% oxygen
Inspired oxygen • No difference in the incidence of postoperative atelectasis if nitrous oxide in oxygen was used or if air in oxygen was used • The very rare possibility of acute hypoxemia in the event of difficulty with airway management versus the common and predictable — but generally mild—impact of hyperoxia-induced atelectasis on later intraoperative gas exchange • A lower FIO2 to replace preoxygenation has not been recommended
Effects of age • Progressive age is not associated with increased propensity for development of atelectasis • Young children (aged 1–3 yr) develop atelectasis more readily greater thoracic wall compliance, less outwardly directed lung distension forces • Children younger than 2yr prone to respiratory failure and fatigue: type I and II muscle fibers are not fully developed • Infant at greater risk for atelectasis because the elastic supporting structure of the lung is incompletely developed
Body habitus • Obesity markedly reduced FRC and lung compliance development of atelectasis worsens arterial oxygenation • The weight of the torso and abdomen make diaphragmatic excursions more difficult— especially when recumbent or supine—the FRC decreases, intensified in paralysis with neuromuscular blockade • Pregnancy also potentiates atelectasis
Tidal volume • The use of low tidal volume in patients with ARDS reduces stretch-induced lung injury in patients with ARDS, improved patient survival • Low tidal volume increases atelectasis in the absence of lung injury • The specific “low-tidal-volume” approach was actually associated with the development of intrinsic PEEP • Pressure-controlled ventilation results in smaller delivered tidal volumes when respiratory system compliance is decreased may lead to atelectasis and may go undiagnosed
Preexisting lung disease • Smokers and patients with lung disease show more pronounced gas exchange impairment than healthy subjects • Only a small shunt and almost no atelectasis develops in these patients, but they may have severe VA/Q mismatch • COPD may make them resist collapse • Large regions with low VA/Q ratios that can result, over time, in resorption atelectasis
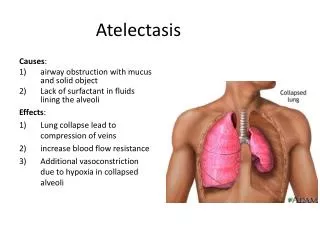
Effects of atelectasis • Decreased compliance • Impaired oxygenation • Pulmonary vascular resistance increase • Lung injury
Postoperative period • Atelectasis can persist for 2 days after major surgery • The lung dysfunction is often transient; may be related to reduction in FRC • Postoperative mechanical respiratory abnormality after abdominal or thoracic surgery is a restrictive pattern with severely reduced inspiratory capacity, vital capacity, and FRC pain control in preventing postoperative atelectasis • Atelectasis and pneumonia are often considered together because the changes associated with atelectasis may predispose to pneumonia
Detection of atelectasis • Conventional chest radiography • Computed tomography • Magnetic resonance imaging • Ultrasonography • Intravital microscopy • Cytokine profile
Prevention / reversal of atelectasis • Healthy lungs • Reversible by passive hyperinflation (i.e., three successive inflations: a pressure of 20cmH2O for 10s; then a pressure of 30cm H2O for 15s; and third, a pressure of 40 cm H2O sustained for 15s) • High initial pressures are needed to overcome the anesthesia-induced collapse and that PEEP of 5cm H2O or more is required to prevent collapse • No evidence of barotrauma or pulmonary complications occurred in the high initial airway pressure
Prevention / reversal of atelectasis • Injured lungs • Large tidal volumes, high peak airway pressures, and end-expiratory alveolar collapse with cyclic reopening have all been proposed as deleterious • Calculated the inflection point from a pressure–volume curve, and PEEP was preset at 2cm H2O above the inflection point • Recruiting maneuver: continuous positive airway pressures of 35–40cm H2O for 40 s followed by a return to previous PEEP levels • Optimum overall cardiopulmonary interaction • Only in patients with early ARDS
Treating atelectasis in the postoperative period • Encourage or force patients to inspire deeply • Method: intermittent positive-pressure breathing, deep-breathing exercises, incentive spirometry, and chest physiotherapy • A simple posture change from supine to seated • Thoracic or sternal traction, the use of intravenous aminophylline as successful treatments of atelectasis in a number of case reports
پایگاه پاورپوینت فارسیwww.txtzoom.comبانک اطلاعات هوشمند اسلاید