Download
1 / 22
240 likes | 992 Views
OPEN ANGLE GLAUCOMA Frank J. Weinstock , MD, FACS Professor of Ophthalmology- NEOUCOM Canton, Ohio USA. TYPES OF GLAUCOMA. PRIMARY CHRONIC SIMPLE OPEN ANGLE ANGLE CLOSURE- NARROW ANGLE SECONDARY TRAUMATIC. PRIMARY CHRONIC SIMPLE OPEN ANGLE GLAUCOMA. SERIES OF CONDITIONS

E N D
OPEN ANGLE GLAUCOMAFrank J. Weinstock, MD, FACSProfessor of Ophthalmology- NEOUCOMCanton, OhioUSA
TYPES OF GLAUCOMA • PRIMARY CHRONIC SIMPLE OPEN ANGLE • ANGLE CLOSURE- NARROW ANGLE • SECONDARY • TRAUMATIC
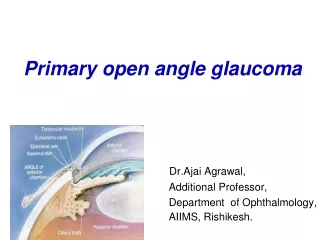
PRIMARY CHRONIC SIMPLE OPEN ANGLE GLAUCOMA • SERIES OF CONDITIONS • OPTIC NERVE AND VISUAL FIELD LOSS SECONDARY TO ELEVATED INTRAOCULAR PRESSURE OR POOR NUTRITION TO OPTIC NERVE • ETIOLOGY- NOT TRULY KNOWN
VARIANTS • TRAUMATIC • SECONDARY • LOW TENSION
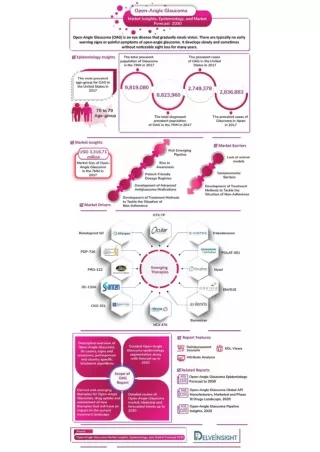
OPEN ANGLE GLAUCOMA • US- 2.2 MILLION (3.4 MILLION BY 2020) • 175000 IN US BLIND (10% OF BLINDNESS) • BLACKS-HISPANICS (30% OF BLINDNESS) • 1 IN 1000 OVER 40 YR OLD- BLIND • OVER 75 YEARS- 2.7/1000 BLIND (6.7/1000 VISUALLY IMPAIRED)
COMPLIANCE • SCREENING $60/SCREENING AND $1000/CASE DISCOVERED • (SCREEN HIGH RISK-RELATIVES-AFRICAN AMERICANS-HISPANICS-) • 25-40% OF PTS. TAKING Rx TO STORE- DON’T PICK IT UP • 60% PICKING UP Rx D/C XALATAN DURING YR AND 76% WITH OTHER MEDS
DIAGNOSIS • OPTIC NERVE FIBER EVALUATION (OPHTHALMOCSCOPE) • VISUAL FIELD EVALUATION- OFFICE • OPTIC NERVE IMAGING AND ANALYSIS- OFFICE • MEASUREMENT OF INTRAOCULAR PRESSURE (PORTABLE) • MEASUREMENT OF CORNEAL THICKNESS • GENETIC PREDISPOSITION ????
SCREENING • OPTIC NERVE EVALUATION- OPHTHALMOLOSCOPE • INTRAOCULAR PRESSURE (IOP) MEASUREMENT- APPLANATION TYPE TONOMETER • IOP HAS DIURNAL VARIATION
GOALS OF SCREENING • EDUCATION • DETECTION OF GLAUCOMA (NOT PROVEN) • TESTS NOT SPECIFIC OR SENSITIVE SCREENING- NO VALUE IF: NOT ABLE TO REFER FOR DEFINITIVE DIAGNOSIS, TREATMENT AND FOLLOWUP
SCREENING • CHOOSE HIGH RISK GROUPS E.G. HISPANICS, BLACKS (OVER AGE 40, WHITES (OVER 65 YEARS OLD), HISTORY OF EYE TRAUMA; DIABETICS; • FAMILY HISTORY OF GLAUCOMA • DIABETICS • PATIENTS WITH SEVERE MYOPIA
INTRAOCULAR PRESSURE • VERY EASY TO DO- PORTABLE INSTRUMENTS • POOR SENSITIVITY AND SPECIFICITY • NORMAL- 20 mmHg OR LESS • MEASURED BY: APPLANATION TONOMETER- NOT PRACTICAL • FINGER PALPATION- INACCURATE APPLANATION TONOMETRY
SCHIOTZ TONOMETER ADVANTAGES: INEXPENSIVE PORTABLE EASY TO USE READILY AVAILABLE DISADVANTAGES: NOT THE MOST ACCURATE REQUIRES TOPICAL ANESTHETIC
OPHTHALMOSCOPY • EASY; QUICK • REQUIRES OPHTHALMOSCOPE- AVAILABLE • REQUIRES EXPERT AT OPHTHALMOSCOPY • PICKS UP DEFINITIVE GLAUCOMA ( A LATE STAGE)- MAY BE TOO LATE TO HAVE MUCH BENEFIT • INTER-OBSERVER VARIABILITY • NORMAL C:D RATIO- 0.3 OR LESS THAN 0.2 DIFFERENCE • (STEREO VIEWS ARE BEST (NOT PRACTICAL)
E-11 Normal and Cupped Disc NORMAL CUPPED DISC ENLARGED CUP
PERIPHERAL VISUAL FIELD TESTING • PICKS UP LATER GLAUCOMA • REQUIRES EXPENSIVE EQUIPMENT- DIFFICULT TO PERFORM- NOT PRACTICAL FOR SCREENING • OPTIC NERVE ANALYSIS- PICKS UP PROBLEMS EARLIER (REQUIRES EXPENSIVE EQUIPMENT AND TECHNNICAL SUPPORT)- NOT PRACTICAL FOR SCREENING
REFERRAL • SET CRITERIA FOR EACH SCREENING • E.G PRESSURE OVER 20 MM hG • INDIVIDUALS WITH SUSPICIOUS DISCS (LARGE CUPS) • OPTIC NERVE- HEMORRHAGES; LARGE CUP:DISC RATIO (OVER 0.4) OR ASYMMETRY OF CUPS (HORIZONTAL AND VERTICAL CUP:DISC RATIO)- 0.3 DIFFERENCE
BEST SCREENING • COMPREHENSIVE EYE EXAM IN OFFICE SETTING- BY SPECIALIST
ADDITIONAL SCREENING BENEFITS • POSSIBLY MORE IMPORTANT THAN DIAGNOSING GLAUCOMA • EDUCATION OF NEED FOR EYE CARE • OPHTHALMOSCOPIC EXAM WILL PICK UP: • CATARACTS • CORNEAL SCARS • RETINAL DISEASE- DIABETES, HYPERTENSION, TUMORS
TREATMENT OF GLAUCOMA • MEDICATIONS- MANY NEW MEDICATIONS- POTENTIAL SIDE-EFFECTS • ONCE A DAY DOSAGE- BEST COMPLIANCE • TREAT EARLIER • LASER OR SURGERY- EARLIER ????- BEING EVALUATED • WHICH FIRST? – BEING EVALUATED • NEW PROCEDURES • GOAL- < 20mmHg. (LOWER IN MANY SITUATIONS)
SUMMARY • GLAUCOMA SCREENING • QUESTIONNABLE BENEFIT FOR PREVENTING BLINDNESS • WILL PICK UP A NUMBER OF CASES GLAUCOMA AND OTHER EYE CONDITIONS • CONCENTRATE ON HIGH-RISK GROUPS • EASY TO DO • MARKED EDUCATIONAL AND PUBLIC RELATIONS BENEFIT