Download

1 / 22
230 likes | 759 Views
Previous IARC Monographs on Formaldehyde. Vol 29, 1981: inadequate evidence in humans, sufficient evidence in animals (2B) Suppl1,1987: limited evidence in humans, sufficient evidence in animals, 2A

E N D
Previous IARC Monographs on Formaldehyde • Vol 29, 1981: inadequate evidence in humans, sufficient evidence in animals (2B) • Suppl1,1987: limited evidence in humans, sufficient evidence in animals, 2A • Vol 62, 1994: limited evidence in humans, sufficient evidence in animals, 2A
Reasons for re-evaluation IARC Monographs Advisory Group (Feb 2003) on priorities for future evaluations • New epidemiological studies available, two more will be finished soon • Complex mechanistic data High priority for re-evaluation
The IARC Monographs • Examination of all relevant information to assess the weight of the evidence that certain exposures could alter the incidence of cancer in humans. • Do not include quantitative extrapolation of experimental data to humans. • Do not include recommendations regarding regulation or legislation (responsibility of individual governments & other international organizations.)
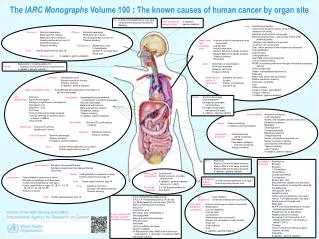
Nasopharyngeal Cancer (NPC) - I US NCI Cohort among formaldehyde workers • Statistically significant excess of deaths from NPC in largest & most informative cohort study of industrial workers(8 deaths, SMR 2.10, 95%CI 1.05-4.21) • Statistically significant exposure–response relationships for peak (ptrend < 0.001) and cumulative exposure(ptrend = 0.03)
Nasopharyngeal Cancer (NPC) - II Other cohort studies • Excess of deaths in largest US cohort of embalmers(4 obs, 1.83 expected) (Hayes et al, 1990) • Excess risk among workers using or manufacturing formaldehydein Denmark (SPIR 1.3, 95%CI 0.3-3.2) (Hansen and Olsen, 1995) • 3 other cohort studies (US garment manufacturers, British chemical workers & US embalmers) with fewer cases than expected, but low statistical power (Pinkerton et al, 2004; Coggon et al, 2003; Walrath et al, 1983)
Nasopharyngeal Cancer (NPC) - III Case-control studies • 5 of 7 case–control studies found increased risk for overall exposure to formaldehyde, or in higher exposure categories, including one with statistically significantincrease in risk • 3 case–control studies (2 published since the last Monograph) found higher risks in subjects with the highest probability, level or duration of exposure
Nasopharyngeal Cancer (NPC) - IV Meta-analysis Most recent meta-analysis (Collins 1997) • included some but not all of the above studies • increased overall meta-relative risk for nasopharyngeal cancer (RR 1.3, 95%CI 1.2-1.5)
Leukemia - I • Excess mortality observed consistently (6 of 7 studies) among professional workers: embalmers, funeral parlour workers, pathologists and anatomists • Recent meta-analysis for exposure to formaldehyde among professionals (Collins 2004):increased overall summary relative risk estimates for embalmers (RR 1.6, 95%CI 1.2-2.0), and for pathologists & anatomists (RR 1.4, 95%CI 1.0-1.9) • Predominantly myeloid leukemia
Leukemia - II • Little direct evidence that these professionals have a higher incidence of viral infections or that viruses have a causal role in myeloid leukemia • No material exposure to known leukemogens
Leukemia - III • Statistically significant exposure–response relationship between peak exposures to formaldehyde and leukemia in cohort of U.S. industrial workers (RR 2.5 95%CI 1.3-4.6) (Hauptmann et al, 2003) • Relationship particularly strong for myeloid leukemia (RR 3.5 95%CI 1.3-9.4) • Mortality from leukemia less than expected when compared with general population as the referent • No exposure–response relationship with cumulative exposure - other metrics may be more relevant?
Leukemia - IV • Excess mortality from leukemia among entire cohort of US garment workers (Pinkerton et al, 2004) • Excess somewhat stronger for myeloid leukemia • Excess stronger among workers with long duration of exposure and long follow-up, who had been employed early in the study period when exposures to formaldehyde were believed to be the highest
Leukemia - V • No excess mortality among British industrial workers exposed to formaldehyde - difficult to reconcile with positive studies • No evaluation of peak exposures • Nospecific examination of myeloid leukemia
Sinonasal cancer - I • Pooled analysis of 12 occupational case–control investigations (Luce et al, 2002) • Increased risk for adenocarcinoma after adjustment for known occupational confounders • Increased risk among subjects never occupationally exposed to wood or leather dust(small number of exposed cases) • Dose–response trend for cumulative exposure • Little evidence of association with SCC
Sinonasal cancer - II • Increased risk of sinonasal cancer (particularly SCC) in one other case–control study & among industrial workers in Denmark (proportionate incidence study) (Olsen et al, 1986; Hansen et al, 1995) • No excess of sinonasal cancer in recently updated industrial cohort studies
Sinonasal cancer - III • Most studies have not distinguished tumours arising in the nose from those developing in the nasal sinuses - effect on the risk of nasal cancer would be diluted if there were no corresponding effect on the risk of cancer in the sinuses • Discrepancy between results of case–control and cohort studies might also reflect residual confounding by wood dust in the former
Overall evaluation • Formaldehyde is carcinogenic to humans, Group 1 • Sufficient evidence in humans that formaldehyde causes nasopharyngeal cancer • Strong but not sufficient evidence for a causal association between leukemia and occupational exposure to formaldehyde • Limited evidence in humans that formaldehyde causes sinonasal cancer.
Publications • VJ Cogliano, Y Grosse, RA Baan, K Straif, MB Secretan, F El Ghissassi. Advice on formaldehyde and glycol ethers. The Lancet Oncology 2004, 5:528 • VJ Cogliano, Y Grosse, RA Baan, K Straif, MB Secretan, F El Ghissassi, and the Working Group for Volume 88*. Meeting report: summary of IARC Monographs on formaldehyde, 2-butoxyethanol and 1-tert-butoxy-2-propanol. Environ Health Perspect 2005, 113: 1205 –8 *Ulrich Andrae, Germany, Sherwood Burge, UK. Rajendra Chhabra, USA, John Cocker, UK, David Coggon, UK, Rory Conolly, USA, Paul Demers, Canada, David Eastmond, USA, Elaine Faustman, USA, Victor Feron, The Netherlands, Michel Gérin, Canada (Chair) Marcel Goldberg, France, Bernard Goldstein, USA, Roland Grafström, Sweden, Johnni Hansen, Denmark, Michael Hauptmann, USA, Kathy Hughes, Canada, Ted Junghans, USA, Dan Krewski, Canada, Steve Olin, USA, Martine Reynier, France, Judith Shaham, Israel, Morando Soffritti, Italy, Leslie Stayner, USA, Patricia Stewart, USA, Douglas Wolf, USA,
Summary of relevant data for evaluating carcinogenicity 1. Exposure information 2. Reports of carcinogenicity in humans 3. Reports of carcinogenicity in experimental animals 4. Other data relevant to the evaluation of carcinogenicity and its mechanisms
Carcinogenicity in humans Sufficient evidence of carcinogenicity The Working Group considers that a causal relationship has been established between exposure to the agent, mixture, or exposure circumstance and human cancer. A positive relationship has been observed between the exposure and cancer in studies in which chance, bias and confounding could be ruled out with reasonable confidence
Other data relevant to an evaluation of carcinogenicity and its mechanisms • Evidence of genotoxicity (structural changes at the gene level) • Evidence of effects on relevant gene expression (functional changes at the intracellular level • Evidence of relevant effects on cell behavior (morphologic or behavioral changes at the cellular or tissue level); • Evidence from dose and time relationships of carcinogenic effects and interactions between agents