Download
1 / 10

E N D
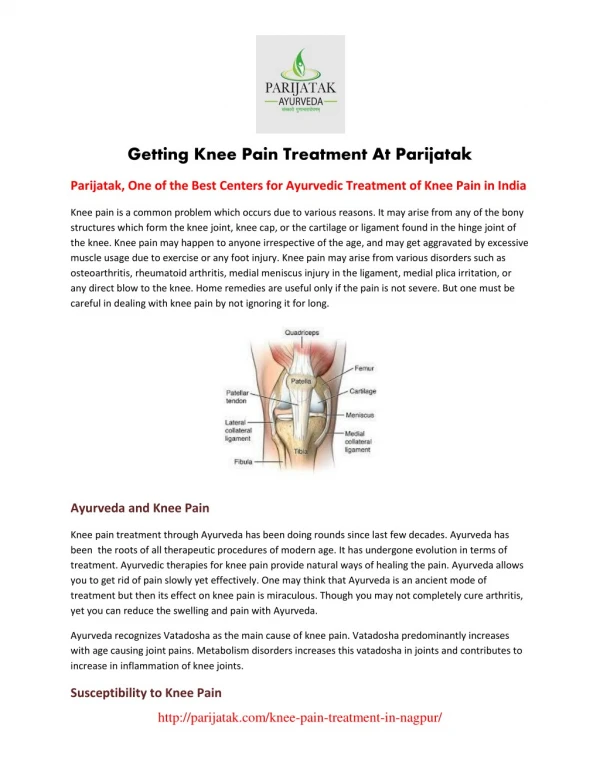
Knee Pain Overview Introduction to Knee Pain Knee pain is the most common musculoskeletal complaint that brings people to their doctor.With today's increasingly active society, the number of knee problems is increasing. Kneepain has a wide variety of specific causes and treatments. Anatomy of the Knee The knee joint's main function is to bend, straighten, and bear the weight of the body,along with the ankles and hips. The knee, more than just a simple hinged joint, however,also twists and rotates. In order to perform all of these actions and to support theentire body while doing so, the knee relies on a number of structures including bones,ligaments, tendons, and cartilage. Bones The knee joint involves four bones. The thighbone or femur comprises the top portion of the joint. One of the bones in the lower leg (or calf area), the tibia, provides the bottom weight-bearing portion of the joint. The kneecap or patella rides along the front of the femur. The remaining bone in the calf, the fibula, is not involved in the weight-bearing portionof the knee joint but provides ligament attachments for stability. Ligaments Ligaments are dense fibrous bands that connect bones to each other. The knee includes four important ligaments, all of which connect the femur to the tibia: The anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) provide frontand back (anterior and posterior) and rotational stability to the knee. The medial collateral ligament (MCL) and lateral collateral ligament (LCL) located alongthe inner (medial) and outer (lateral) sides of the knee provide medial and lateralstability to the knee. Tendons Tendons are fibrous bands similar to ligaments. Instead of connecting bones to other bones as ligaments do, tendons connect muscles tobones. The two important tendons in the knee are (1) the quadriceps tendon connecting thequadriceps muscle, which lies on the front of the thigh, to the patella and (2) thepatellar tendon connecting the patella to the tibia (technically, this is a ligamentbecause it connects two bones). The quadriceps and patellar tendons are sometimes called the extensor mechanism, andtogether with the quadriceps muscle they facilitate leg extension (straightening). Cartilage Cartilaginous structures called menisci (singular form is "meniscus") line the top of thetibia and lie between the tibia and the 2 knuckles at the bottom of the femur (called thefemoral condyles).
The menisci's primary job is to provide cushioning for the knee joint. Bursae Bursae (one is a bursa) are fluid-filled sacs that help to cushion the knee. The kneecontains 3 important groups of bursae: The prepatellar bursae lie in front of the patella. The Pes anserine bursae is located on the inner side of the knee about 2 inches below thejoint. The infrapatellar bursae are located underneath the patella. Home Care for Knee Pain Inflammation is the body's physiologic response to an injury. In treating many types ofknee pain, a common goal is to break the inflammatory cycle. The inflammatory cycle startswith an injury. After an injury, substances that cause inflammation invade the knee toassist in healing. However, if the injury and subsequent inflammation is not resolved,inflammation can become a chronic issue, leading to further inflammation and additionalinjury. This cycle of inflammation leads to continued or progressive knee pain. The cyclecan be broken by controlling the substances that cause inflammation, and by limitingfurther injury to tissue. Some common home care techniques for knee pain that control inflammation and help to breakthe inflammatory cycle are protection, rest, ice, compression, and elevation. This regimenis summarized by the memory device PRICE. PROTECT the knee from further trauma. This can be done with knee padding or splinting. A pad over the kneecap, for example, helps to control the symptoms of some knee injuries(an example is a form of bursitis sometimes called housemaid's knee) by preventing furtherrepetitive injury to the prepatellar bursae. REST the knee. Rest reduces the repetitive strain placed on the knee by activity. Rest both gives the knee time to heal and helps to prevent further injury. ICE the knee. Icing the knee reduces swelling and can be used for both acute and chronic knee injuries. Most authorities recommend icing the knee 2 to 3 times a day for 20-30 minutes each time. Use an ice bag or a bag of frozen vegetables placed on the knee. COMPRESS the knee with a knee brace or wrap. Compression reduces swelling. In some knee injuries, compression can be used to keep the patella aligned and to keepjoint mechanics intact. ELEVATE the knee. Elevation also helps reduce swelling.
Elevation works with gravity to help fluid that would otherwise accumulate in the kneeflow back to the central circulation. Prop your leg up when you are sitting, or use a recliner, which naturally elevates thelegs. Elevation works best when the knee-- or any other injured body part-- is higher thanthe level of the heart. Over-the-counter pain medicine: Commonly used pain relievers, such as nonsteroidal anti-inflammatory drugs (NSAIDs) like naproxen (Aleve or Naprosyn) and ibuprofen (Advil orMotrin), also play a role in the treatment of knee pain. These drugs directly control pain and, at higher doses, act as anti-inflammatory agents,helping to break the inflammatory cycle. Like all medications, however, these drugs haveside effects. You should not use NSAIDs if you have a problem with bleeding or stomach ulcers or sometypes of kidney disease. Acetaminophen (Tylenol) can also be used to control knee pain but does not have the anti-inflammatory properties of the NSAIDs. Still, this treatment is remarkably useful in manytypes of knee pain, such as osteoarthritis. When to Call the Doctor for Knee Pain When you are deciding whether to call the doctor about your knee pain, a good rule ofthumb exists for most long-term knee injuries. If your symptoms have not gone away aftertrying a week of PRICE therapy and over-the-counter anti-inflammatory pain meds, youshould set up an appointment with your doctor, physical therapist, or a sports medicineorthopaedic (bone and muscle) specialist to further evaluate the pain. This rule can alsobe applied to new knee injuries that are not disabling. Remember, however, that this ruleshould only serve as a guide. If you are concerned about the pain, you should call thedoctor. When to Go to the Hospital for Knee Pain If you can not put weight on your knee, feel sick, or have a fever or if your knee is redand hot, you should consider going to the ER to be evaluated by a doctor because of thepossibility of a fracture or infection. Many fractures may require immobilization in a specific position or surgery. Infections need immediate attention. They can be managed but require prompt care. Putting off seeing a doctor may hinder healing. Other signs and symptoms that demand emergency evaluation: Unbearable pain Pain that does not improve with rest Pain that wakes you Drainage Large wounds Puncture wounds Swelling, if you are on a blood thinner (warfarin or Coumadin) or have a bleeding disorder(such as hemophilia). Getting a Knee Pain Diagnosis.
History: Even in today's world of technology, doctors rely on a detailed history andphysical exam more than any single test. The doctor will typically want to know the exact nature of the pain. Where in the knee is your pain? What does the pain feel like? How long has the pain been present? Has it happened before? Describe any injuries to the knee. What makes it better or worse? Does the knee pain wake you up at night? Does the knee feel unstable? Have you been limping? The doctor will also want to know a bit about you. Do you have any major medical problems? How active is your lifestyle? What are the names of the medications you are taking? The doctor will want to know about any related symptoms. Do you still have normal sensation in your foot and lower leg? Have you been having fevers? Physical exam. The doctor will likely have you disrobe to completely expose the knee. If possible, wearshorts to your appointment. The doctor will then inspect the knee and press around the knee to see exactly where it istender. In addition, the doctor may perform a number of maneuvers to stress the ligaments,tendons, and menisci of the knee and evaluate the integrity of each of these. X-rays, CT scans, and other tests. Depending on your particular history and exam, the doctor may suggest X-rays of the knee.X-rays show fractures (broken bones) and dislocations of bones in the knee as well asarthritis and abnormally large or small joint spaces. Rarely, the doctor may order a CT scan (a 3-dimensional X-ray) of the knee to preciselydefine a fracture or deformity. Both X-rays and CT scans are excellent for diagnosing fractures. They both are also poor,however, at evaluating soft tissue structures of the knee, such as ligaments, tendons, andthe menisci. MRI. Magnetic resonance imaging (MRI) uses large magnets to create a 3-dimensional image of theknee. In contrast to CT scans, MRIs do not image bones and fractures. However, they areexcellent for evaluating ligaments and tendons. Fluid removal.
The knee and all bursae of the knee are filled with fluid. If your symptoms suggest infection or crystalline arthritis, such as gout, your physicianmay remove fluid, with a needle, from the knee. This fluid will then be analyzed to better clarify the diagnosis. Crystals, which suggest crystalline arthritis, often can be seen under the microscope.Infection may also be detected under a microscope by finding bacteria and pus in thefluid. The doctor may also elect to perform certain blood tests to evaluate for signs ofinfection or diseases such as rheumatoid arthritis, lupus, and diabetes. Arthroscopy. The orthopedic surgeon may elect to perform arthroscopy if you have chronic knee pain. This is a surgical procedure where the doctor will place a fiber optic telescope withinthe knee joint. The arthroscope is attached to a camera that relays real-time images to avideo monitor. By doing so, the surgeon may be able to see small particles in the knee or to look moreclosely at damaged menisci or cartilage. The doctor may also be able to treat damage by shaving down torn cartilage or removingparticles from the knee while looking at the inside of your knee on a video monitor. Types of Knee Pain The nerves that provide sensation to the knee come from the lower back and also providehip, leg, and ankle sensation. Pain from a deeper injury (called referred pain) can bepassed along the nerve to be felt on the surface. Knee pain, therefore, can arise from theknee itself or be referred from conditions of the hip, ankle, or lower back. All of thefollowing sources of knee pain arise from the knee joint itself. In general, knee pain is either immediate (acute) or long-term (chronic). Acute knee painscan be caused by an acute injury or infection. Chronic knee pain is often from injuries orinflammation (such as arthritis) but can also be caused by infection. Acute Knee Pain Sprained and Torn Cruciate Ligaments Description: An anterior cruciate ligament (ACL) injury is a common sports injurygenerally caused by a hard stop or a violent twisting of the knee. The posterior cruciateligament (PCL) is stronger than the ACL and much less commonly torn. A PCL injury mayhappen with a serious blow, such as when the knee strikes the dashboard in a car accident;this is why a PCL injury is often associated with other ligament and bone injuries. Symptoms: If you tear your ACL, you may hear a pop. You will also notice your knee giveway or become unstable and feel pain that is bad enough that you might feel like vomiting.This will, almost always, be followed by marked knee swelling over the next couple ofhours because the ACL bleeds briskly when torn.
Treatment: Surgical repair is often recommended for high-level athletes who demand optimaloutcomes. Conservative treatment and knee braces may prove sufficient for those who do notdemand quite so much from their knees. Tendon Ruptures Description: Both the quadriceps and patellar tendons may rupture partially or completely.A quadriceps tendon rupture typically occurs in recreational athletes older than 40 years(this is the injury former President Clinton suffered while jogging), and a patellartendon rupture typically occurs in younger people who have had previous tendonitis orsteroid injections to the knee. Symptoms: Rupture of either the quadriceps or patellar tendon causes pain (especially whentrying to kick or extend the knee). Those people with complete ruptures are unable toextend the knee. The patella is also often out of place either upward (with patellartendon rupture) or downward (with quadriceps tendon rupture). Treatment: Tendon ruptures require urgent care. They typically need surgical repair, whilea partial rupture may be treated with splinting alone. Meniscal Injuries Description: Injuries to the meniscus are typically traumatic injuries but can also be dueto overuse. Often, a piece of the meniscus will tear off and float in the knee joint. Symptoms: Meniscal injuries may cause the knee to lock in a particular position, or eitherclick or grind through its range of motion. Meniscal injuries may also cause the knee togive way. Swelling typically accompanies these symptoms, although the swelling may be muchless severe than with an ACL injury. Treatment: Meniscal injuries often require arthroscopic surgical repair. A locking knee ora knee that "gives" should be evaluated for arthroscopic repair. Knee Dislocation Description: Knee dislocation is a medical emergency. Dislocation of the knee is caused bya particularly powerful blow to the knee. The lower leg becomes completely displaced withrelation to the upper leg. This displacement stretches and frequently tears not only theligaments of the knee but also arteries and nerves. Untreated arterial injuries leave thelower leg without a blood supply. If circulation is not restored, amputation may berequired. Nerve injuries, on the other hand, may leave the lower leg viable but withoutstrength or sensation. Symptoms: Knee dislocations are severely painful and produce an obvious deformity of theknee. Many dislocations are reduced-- or put back into alignment-- on their own. As thisoccurs, many will report feeling a dull clunk. Treatment: If the knee dislocation has not been put back into place on its own, the doctorwill immediately reduce the dislocation. Medical treatment, however, does not stop here.Whether a dislocation reduces by itself or is put back into place in the hospital, itrequires further evaluation and care. After reduction, people with these injuries areobserved in the hospital where they usually do a number of tests to ensure that noarterial or nerve injury has occurred. If such an injury is found, it must be repairedimmediately in the operating room.
Dislocated Kneecap (patella). Description: A common injury caused by direct trauma or forceful straightening of the leg,such as an injury that happens when serving in volleyball or tennis. Kneecap dislocationis more common in women, the obese, knock-kneed people, and in those with high-ridingkneecaps. Symptoms: If you have this injury, you will notice the patella being out of place and mayhave difficulty flexing or extending your knee. Treatment: The doctor will move the patella back into place (reduce the dislocation). Evenif the patella goes back into place by itself, it needs to be X-rayed for a fracture.After reducing the dislocation and ensuring the absence of a fracture, the doctors willtreat these injuries by splinting the knee to allow the soft tissues around the patella toheal followed by strengthening exercises to keep the patella in line. This injury oftencauses damage to the cartilage on the back of the patella. Chronic Knee Pain Arthritis: Arthritis of the knee is an inflammatory disorder of the knee joint that isoften painful. Arthritis has many causes. Knee Osteoarthritis Description: Osteoarthritis (OA) is caused by degeneration of cartilage in the knee. Inits extreme form, the menisci (cartilage) will be completely eroded, and the femur willrub on the tibia, bone on bone. Symptoms: Osteoarthritis causes a chronically painful knee that is often more painful withactivity. Treatment: Treatment is aimed at pain control with over-the-counter pain relievers. Anti-inflammatory medications, either over-the-counter or by prescription, can be helpful.Hyaluronic acid, a lubricating gel, often injected into the knee over a course of 3-6weeks, can provide substantial relief for one year or more. Severe OA can be treated withnarcotic pain medicines or a knee joint replacement in which a synthetic joint replacesyour knee joint. Additionally, physical therapy to manage OA pain and knee function can bebeneficial. Rheumatoid Arthritis of the Knee Description: Rheumatoid arthritis (RA) is a connective tissue disease of the whole bodythat affects many joints, often the knee. Symptoms: In addition to knee pain, rheumatoid arthritis may produce morning stiffness andpain in other joints. Treatment: Treatment includes pain medications, anti-inflammatory medications, andprescription drugs (such as Rheumatrex) that are aimed at slowing disease progression. Crystalline Arthritis (gout and pseudogout). Description: These severely painful forms of arthritis are caused by sharp crystals thatform in the knee and other joints. These crystals can form as a result of defects in theabsorption or metabolism of various natural substances such as uric acid (which producesgout) and calcium pyrophosphate (pseudogout).
Treatment: Treatment is aimed at controlling inflammation with anti-inflammatorymedications, and at aiding the metabolism of the various chemicals that may lead tocrystal formation. Bursitis. Description: As a result of trauma, infection, or crystalline deposits, the various bursaeof the knee may become inflamed. Symptoms: Acute or chronic trauma causes a painful and often swollen knee from theinflammation of the bursae. A particularly common bursitis is prepatellar bursitis. Thistype of bursitis occurs in people who work on their knees. It is often referred to ashousemaid's knee or carpet layer's knee. Another type of bursitis is anserine bursitis.The anserine bursa is located about 2 inches below the knee along the medial side of theknee. More commonly occurring in the overweight and in women, but also affecting athletesand others, anserine bursitis often causes pain in the region of the bursa and is oftenworse with bending the knee or at night with sleep. Treatment: Treatment will usually include home care with PRICE therapy and NSAIDs. Severeforms, however, can be treated with periodic steroid injections. Infection (or infectious arthritis). Description: Many organisms may infect the knee. Gonorrhea, a common sexually transmitteddisease, can infect the knee, as can common organisms residing on normal skin. Symptoms: Infection of the knee causes painful knee swelling. In addition, people whodevelop such infection typically complain of fevers and chills. Less severe infections maynot have associated fevers. Treatment: New swelling and pain in the knee must be evaluated for infection by a doctor.Treatment usually includes intensive antibiotic therapy. Aspiration of the joint orsurgical drainage may also be recommended. Patellofemoral Syndrome and Chondromalacia Patella. Description: These two conditions represent a continuum of diseases caused by patellarmistracking. Symptoms: The conditions typically occur in young women, in athletes of both sexes, and inolder people. In patellofemoral syndrome, the patella rubs against the inner or outerfemur rather than tracking straight down the middle. As a result, the patellofemoral jointon either the inner or outer side may become inflamed, causing pain that is worse withactivity or prolonged sitting. As the condition progresses, softening and roughening ofthe articular cartilage on the underside of the patella occurs, leading to chondromalaciapatella. Treatment: Home care with PRICE therapy, NSAIDs, and exercises (such as straight legraises) that balance the muscles around the patella work for most people. Physical therapyto assess factors that may contribute to the disease process guides management to includeexercise, bracing or taping of the patella, commercial arch supports (for the arch of thefoot), or orthotic supports that correct foot mechanics and may reduce abnormal forces onthe knee. Severe cases of patellofemoral
syndrome or chondromalacia may be treatedsurgically through a variety of procedures. Jumper's Knee. Description: Tendonitis (inflammation of the tendon) of the quadriceps tendon at the upperpoint of the patella, where it inserts, or tendonitis of the patellar tendon either at thelower point of the patella, or at the place where it inserts on the tibia (called thetibial tuberosity, the bump is about 2 inches below the knee on the front side). Jumper'sknee is so named because it is typically seen in basketball players, volleyball players,and people doing other jumping sports. Symptoms: Jumper's knee causes localized pain that is worse with activity. It usuallyhurts more as you jump up than when you land, because jumping puts more stress on tendonsof the knee. Treatment: Home therapy with the PRICE regimen, along with anti-inflammatory drugs, is thebasis of treatment to manage the acute phase. Particularly important are rest, ice, andNSAID drugs, which will help stop the pain and break the cycle of inflammation. Aftercontrolling the pain, you should slowly start an exercise regimen to strengthen thequadriceps, hamstrings, hip, and calf muscles before resuming your sport of choice a fewweeks down the line. Also, bracing of the extensor mechanism may help remove stress fromthe tendons. Osgood- Schlatter Disease. Description: Osgood-Schlatter disease occurs in adolescent athletes where repetitiveextension of the knee causes inflammation and injury of the tibial tubercle (the bonyprotrusion at the top of the shin, just below the kneecap). Symptoms: Children suffering from this syndrome report pain at the tibial tubercle. Thispain is typically worse when extending the leg. The tibial tubercle is tender to touch andover time begins to protrude more because the chronic inflammation stimulates the bone togrow. Treatment: Osgood-Schlatter disease is a self-limited condition that usually resolves asthe the tibial tubercle stops growing with the end of adolescence (at about age 17 inmales and age 15 in females). Treatment includes PRICE and NSAID therapy to minimize acutepain from activity. Physical therapy to identify limitations will reduce stress to thetibial tubercle and often includes strength training of the hip and core. In severe cases,splinting the knee for a few weeks may help reduce the pain and halt the inflammationcycle. Iliotibial Band Syndrome. Description: A fibrous ligament, called the iliotibial band, extends from the outside ofthe pelvic bone to the outside of the tibia. When this band is tight it may rub againstthe bottom outer portion of the femur (the lateral femoral condyle). Symptoms: Distance runners typically suffer from this condition. These runners complain ofoutside knee pain usually at the lateral femoral condyle. Early on, the pain willtypically come on 10 minutes to 15 minutes into a run and improve with rest.
Treatment: The most important aspect of treating iliotibial band syndrome is to identifywhy it is tight. A physical therapist can evaluate mechanics and prescribe treatments,which may include stretching the iliotibial band. One way to do this is to place the rightleg behind the left while standing with your left side about 2 feet to 3 feet from a wall.Then, lean toward your left for 20 to 30 seconds using the wall to help you supportyourself. In addition to stretching the iliotibial band, PRICE therapy and NSAIDs may beof some help. Knee Pain Prevention Knee pain has a host of causes. Many types of pain are difficult to prevent, but you cando some general things to reduce the likelihood of sustaining a knee injury. Stay Slim Staying slim reduces the forces placed on the knee during both athletics and everydaywalking and may, according to some medical research, reduce osteoarthritis. Keeping your weight down may also reduce the number of ligament and tendon injuries forsimilar reasons. Keep Limber, Keep Fit Many knee problems are caused by tight or imbalanced musculature. Stretching andstrengthening, therefore, also help to prevent knee pain. Stretching keeps your knee from being too tight and aids in preventing both patellofemoralsyndrome and iliotibial band syndrome. Strengthening exercises, particularly of the quadriceps (straight leg raises and legextensions are among the prescribed exercises), can help prevent knee injury and areessential to reducing arthritis and associated complications. Exercise Wisely If you have chronic knee pain, consider swimming or water exercises. In water, the forceof buoyancy supports some of our weight so our knees aren't burdened. If you don't have access to a pool or do not enjoy water activities, at least try to limithard pounding and twisting activities such as basketball, tennis, or jogging. You may find that your aching knees will act up if you play basketball or tennis every daybut will not if you limit your pounding sports to twice a week. Whatever you do, respect and listen to your body. If it hurts, change what you are doing. If you are fatigued, consider stopping-- many injuries occur when people are tired. Protect the Knee Wearing proper protection for the activity at hand can help avoid knee injuries. When playing volleyball or when laying carpet, protecting your knees may include kneepads. When driving, knee protection may include wearing a seatbelt to avoid the knee-versus-dashboard injuries as well as injuries to other parts of your body. Visit our website https://nydnrehab.com/what-we-treat/knee-pain/ to make an appointment today.