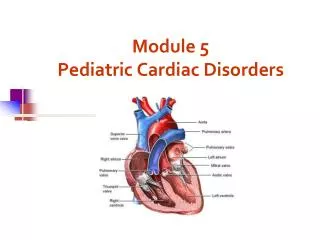
PEDIATRIC INTERVENTIONAL CARDIAC CATHETERIZATION
PEDIATRIC INTERVENTIONAL CARDIAC CATHETERIZATION. Phillip Moore M.D. Department of Pediatrics University of California at San Francisco. Surgery. Interventional Cardiology. CHD - INCIDENCE. VSD 45% PDA 10% Sec ASD 7% PS 7% COARCTATION 6% AS 5% TOF 5% TGA 5%

PEDIATRIC INTERVENTIONAL CARDIAC CATHETERIZATION
E N D
Presentation Transcript
PEDIATRIC INTERVENTIONAL CARDIAC CATHETERIZATION Phillip Moore M.D. Department of Pediatrics University of California at San Francisco
Surgery Interventional Cardiology
CHD - INCIDENCE VSD 45% PDA 10% Sec ASD 7% PS 7% COARCTATION 6% AS 5% TOF 5% TGA 5% Single Ventricle 5% AV Canal 4%
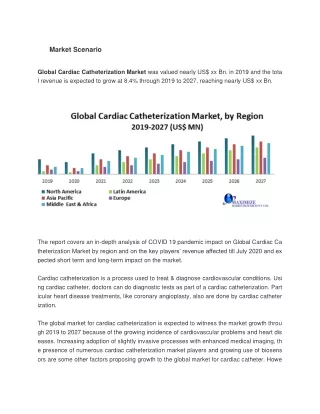
INTERVENTIONAL IMPACT • 0.8 % of all live births have CHD • 32,000 infants / year in U.S.; 15 mil worldwide • 60% require treatment • 19,200 in U.S. / 9 million worldwide • Primary treatment for up to 1/3rd • 6,500 in U.S. / 3 million worldwide • Potential for up to 2/3rds of patients • 13,000 in US / 6 million worldwide
APPROVED PROCEDURES • Balloon Dilation : stenotic valves / vessels • Stent Implantation : stenotic vessels • Coil closure : PDA, cor fistula, collaterals • Device closure : PDA, ASD, PFO, VSD • RF Perforation : Pulm Atresia, restrictive atrial septum in HLH
INVESTIGATIONAL PROCEDURES • Valved Stent Implantation : PI, AI • Covered Stent Implantation : Fontan completion, Shunt palliation • Internal Vessel Band : HLH palliation • Intravascular Suturing : PFO, ASD
PATIENT POPULATION Premature infants and newborns 600 gms to 4 kg to Adolescents and young adults 70 to 100+ kg
CURRENT IMAGING MODALITIES / DRUGS • Radiography / flouroscopy (95+%) • iohexol or iodixanol (max 5 cc / kg / procedure) • Echocardiography (surface, TEE, ICE) • Agitated saline • Optison (rarely)
CATH COMPLICATIONS • 1-2 % major • 7-9 % minor • Risk factors • Age < 2 years • Interventional procedure • Contrast (amount or type) not risk factor • Transient renal failure (dose dependant) • Allergic reaction (non dose dependent)
ADJUNCT IMAGING MODALTIES / DRUGS • MRI / MRA • Gadolinium • Coarctation : Pre and post anatomy and collateral flow • post op TOF / Truncus : RV size and PI
Oblique Sag SE MRA:MIP MRA:VR
ADJUNCT IMAGING MODALTIES / DRUGS • Nuclear Medicine Lung Perfusion Scan • Technesium 99 • Branch PA stenosis flow evaluation - TOF
RADIOGRAPHY LIMITATIONS • Anatomic soft tissue detail poor • Radiation exposure prolonged and repetitive • Expensive non portable equipment
FUTURE CATH IMAGINGMODALITIES / DRUGS • MRI / MRA • Gadolinium, ? • CT - ? • Iomeprol, ? • 3 D Echocardiography - ? • ?
BACKGROUND • MRI - excellent diagnostic / imaging tool • Short bore magnets - access to patients • Shortened sequence / processing times allows for “real time imaging” of the heart
UCSF MRI / CATH LAB Phillips Medical Systems 1.5 T Intera MR Scanner Integris V5000 Digital X ray
MRI Compatable ASD Device Prototype Bucker et al, Proc. Int. Soc. Mag. Reson. Med., 2002
MRI - STENT COMPATABILITY Platinum Nitinol Stainless Steel Fast segmented cine MR (TR/TE 8/3, flip angle=20, slice thickness=10mm)
CONCLUSIONS • Current radiography techniques and agents are safe / useful for peds interventional cath • Advances will require real time 3-D imaging which will come in the form of MRI , CT , or 3-D echo • SAFE and EFFECTIVE contrast agents will be needed in these modalities to allow interventional advances
CHALLENGES • MRI / CT / Echo Compatible Equipment • Faster Acquisition times • Will need 30 frames/sec • Image Resolution • New contrast agents - allow tissue definition to < 2mm (3 mm slices to thick for thin structures)
THE FUTURE IMPROVED CONTRAST AGENTS Interventional cath Real time 3-D imaging Improved Accuracy for Repair of Complex CHD