Download
1 / 21
210 likes | 415 Views
Basic Concepts in Individual and Population Health (3). Intervening on Skin Cancer: a Population Approach. Ian McDowell, Paula Stewart December 2, 2008. Today. Evaluation (RCTs). Individual vs. population approaches. Health promotion. Road map of ideas. Foundations.

E N D
Basic Concepts in Individual and Population Health (3) Intervening on Skin Cancer: a Population Approach Ian McDowell, Paula Stewart December 2, 2008
Today Evaluation (RCTs) Individual vs.populationapproaches Health promotion Road map of ideas Foundations Intro Unit:Health disparities;Determinants; Physician roles Prevention Public health Epidemiololgy& statisticalmethods Scholar; Health Advocate
Case scenario Solar Sally presents with a suspicious skin lesion on her scalp that troubles her mainly because “it looks so gross” • She is a healthy sportswoman who plays “beach”. • Is vague about her use of sunscreen; hats interfere with her volleyball. • She’s in some denial and seems disconnected from concerns over sun exposure. • Referral to dermatologist leads to diagnosis ofmelanoma. • Your options: treat; preach protection; bemoan the foolishness of youth...?
Physician Roles : Options for cancer • Health promotion & population health • Primary prevention • Secondary prevention (screening) • Supportive services – home, community • Treatment – self-care, education, meds, surgery etc. • Rehabilitation • Palliation broad focused
Health Promotion “A process of enabling people to increase control over, and to improve, their health” (WHO) Ottawa Health Promotion Charter(WHO, 1986) • Develop personal knowledge and skills • Create supportive environments • Strengthen community action • Build healthy public policy • Reorient health services During the 1990s, there was a move from Health Promotion to Population Health
Definitions of Population Health • John Frank, 1995: "Population health is a conceptual framework for thinking about why some people, and some peoples, are healthier than others - the determinants of health at individual and population levels. . .” • Health Canada, 1994: "Population health strategies address the entire range of individual and collective factors that determine health, while traditional health care focuses on risks and clinical factors related to particular diseases. Population health strategies are designed to affect the entire population, while health care normally deals with individuals one at a time, usually individuals who already have a health problem or are at significant risk of developing one. . ."
Principles of a Population Health Approach Move upstream from the individual patient; consider the context of the condition • Consider all factors (immediate causes & underlying determinants) • How many people have the problem? • Focus on prevention as well as case management • Use multiple strategies • Involve community in planning programs • Allocate resources on rational basis • Base policies on evidence of effectiveness
Rationale for Population Interventions • Moral arguments: • Duty of society to protect its citizens (public health) • A just society should reduce inequalities in health • Reduce inequities (systematic differences that should not occur) • Economic arguments: • Healthier workforce, more productivity • More taxpayers, greater equity • Reduce health care expenditures • Political arguments: • Stronger nation • Healthy, happy people re-elect their politicians! 8
Why should an MD care about a population approach? • Frustration with always fixing society’s ills: a way to go “upstream”, beyond mere symptomatic treatment of individual patients and tackle root causes • It’s often an efficient use of resources: cost-effective to tackle causes before they produce cases • Moral imperative (“I will ensure that patient well-being is my main focus…”) • May also be more efficient than focusing on severe cases (see next slides)
Health Advocacy for Solar Sally: Who needs to be involved? • The individuals and her family • Health professionals • Sports leaders (coach, etc.) • School or university • Media • General community • City public health officials • Volunteer health organizations (cancer society?) • Business (sun screen manufacturers?) • Government? This is somewhat daunting! Does it need to be coordinated?
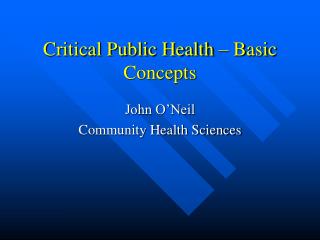
International inequalities in health: survival of children to 5 years of age (vertical axis) plotted by GNI per capita. Source: Gapminder.org
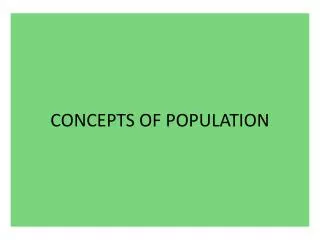
Mortality rates, standardized by age, by income adequacy quintiles, for men (blue) and women (pink) living in the community. Canada 1991 to 2001 Poor Rich Poor Rich
Discussion Point:High risk versus population approach • For every disease, some people are at higher risk than others • We can often recognize such people before the disease occurs; a family physician can readily do this • This “high-risk approach” makes intuitive sense • Are there alternative approaches?
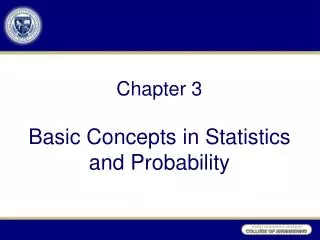
Where Do the Deaths Occur?Example: Serum Cholesterol & CVD Mortality Distribution of serum cholesterol in population Percentage of all CVD deaths 17% 20 8% 22% mortality risk 4% % 10 19% <1% 13% 9% 8% 0 4 5 6 7 8 Serum Cholesterol (mmol/l)
Population changes Example: levels of exercise in a population (red line). To improve population health, you can either focus on encouraging exercise among people who rarely exercise (producing the blue line) Or work to shift whole population distribution (green line). % Low Exercise level High
Types of Preventive Interventions • Active - individual must act to obtain benefit • Voluntary – need education, social norms • supported by legislation • Passive - no action required by individual to obtain benefit • Involuntary • Implemented by policy or legislation
Evaluation • How do we know it works? • Experimental designs • Observational • Statistical aspects will be covered in the tutorial
Experimental Studies:Randomized Controlled Trials People with the diseasewho meet selectioncriteria Interventiongroup (a) (b) Randomallocation Population Controlgroup (c) (d) Time2(outcome) Time1(baseline) Make measurements Statistic = difference in scores = (b-a) - (d-c) This shows the experimental change minus the change in the control group.
Non-random comparison studies People with the diseasewho meet selectioncriteria Interventiongroup (a) (b) Population Controlgroup (c) (d) Time2(outcome) Time1(baseline) Make measurements Statistic = difference in scores = (b-a) - (d-c) This shows the experimental change minus the change in the control group.
A Hierarchy of Quality of Evidence Clinicians should choose therapy according to the best available evidence. To guide you, sources of evidence may be ranked according to their quality. There are various quality rankings; here is one option. In descending order: Level 1: High quality meta-analyses or systematic reviews of RCTs; RCTs with low risk of bias Meta-analyses, systematic reviews, or RCTs with higher risk of bias Level 2: High quality systematic reviews of cohort or case-control studies High quality cohort or case-control studies that had low risk of confounding or bias Level 3: Non-analytic studies (case reports, case series) Level 4: Expert opinion Source: Scottish Intercollegiate Guidelines Network http://www.sign.ac.uk/guidelines/fulltext/50/annexb.html
(Tutorial Groups will discuss design, and evaluation of a health promotion program)