Download
1 / 130
1.56k likes | 2.68k Views
COZAAR (losartan) in Hypertensive Patients with Left Ventricular Hypertrophy. Jeffrey R. Tucker, MD Director, Regulatory Affairs Merck Research Laboratories. The LIFE Study. L osartan I ntervention F or E ndpoint Reduction in Hypertension Study. Dr. J. Tucker, Regulatory Affairs

E N D
COZAAR (losartan) in Hypertensive Patientswith Left Ventricular Hypertrophy Jeffrey R. Tucker, MD Director, Regulatory AffairsMerck Research Laboratories
The LIFE Study Losartan Intervention For Endpoint Reduction in Hypertension Study • Dr. J. Tucker, Regulatory Affairs • Introduction • Dr. J. Edelman, Clinical Development • Background and Rationale • Study Results • Dr. W. Keane, Clinical Development • Review of Evidence and Conclusions Agenda
The LIFE Study Losartan Intervention For Endpoint Reduction in Hypertension Study • Active-control, double-blind • Multicenter • 945 sites • Multinational • 7 countries • Large study population • 9193 hypertensive patients with left ventricular hypertrophy (LVH)
COZAAR (losartan): Proposed New Indication COZAAR is indicated to reduce the risk of cardiovascular morbidity and mortality as measured by the combined incidence of cardiovascular death, stroke, and myocardial infarction in hypertensive patients with left ventricular hypertrophy.
Evidence of Effectiveness from a Single Study • FDA Guidance - Providing Clinical Evidence of Effectiveness for Human Drug and Biological Products (1998) • Generally limited to situations in which a trial shows a benefit on • mortality or irreversible morbidity • the prevention of disease and a second trial is not ethical or practical • Additional information from within the single study, or from other sources, may provide confirmatory evidence to independently substantiate the results of the single study • The LIFE study compared losartan to an active control
The LIFE Study • Study hypothesis: Compared to atenolol, losartan would reduce the incidence of cardiovascular morbidity and mortality in patients with essential hypertension and LVH • The primary endpoint was a composite of cardiovascular morbidity and mortality as measured by the combined incidence of: • Cardiovascular mortality • Stroke • Myocardial infarction • The study evaluated whether a losartan-based regimen would reduce the risk of cardiovascular morbidity and mortality more than an atenolol-based regimen, in the face of comparable blood pressure control in both treatment groups
LIFE: Results • Losartan reduced the risk of the primary composite endpoint (cardiovascular mortality, stroke or MI) • Both the atenolol- and losartan-based regimens reduced blood pressure to a comparable level • The safety profile of losartan was consistent with the currently approved US product circular for COZAAR
Merck Clinical Consultants • Dr. Björn Dahlöf - Chair, Steering CommitteeAssociate Professor of MedicineSahlgrenska University Hospital, Göteborg ,Sweden • Dr. Richard Devereux - Vice Chair, Steering CommitteeProfessor of Medicine and Director Echocardiography Laboratory Cornell Medical Center, New York, NY • Dr. John Kjekshus - Chair, DSMBProfessor of Medicine, Department of CardiologyUniversity of Oslo, Oslo, Norway • Dr. Stevo Julius- US Coordinator, Steering CommitteeProfessor of Medicine, Division of Hypertension and HyperlipidemiaUniversity of Michigan, Ann Arbor • Dr. Peter KoweyProfessor of Medicine, Jefferson Medical CollegeChief, Division of Cardiovascular DiseasesMain Line Hospitals, Philadelphia
Merck Statistical Consultants • Dr. James NeatonProfessor, Division of Biostatistics, School of Public Health, University of Minnesota • Dr. Scott ZegerProfessor and Chair, Department of Biostatistics, Bloomberg School of Public Health, Johns Hopkins University, Baltimore
COZAAR (losartan) in Hypertensive Patientswith Left Ventricular Hypertrophy Jonathan M. Edelman, MD Senior Director, Clinical DevelopmentMerck US Human Health
Losartan in Hypertensive Patients withLeft Ventricular Hypertrophy Agenda • Background and Rationale • LIFE Study Design • LIFE Patient Population • LIFE Efficacy Results • LIFE Safety Results
Hypertension:A Major Public Health Issue • The most common cardiovascular condition in the world • Risk factor for development of cardiovascular, cerebrovascular, renovascular, and peripheral vascular disease • Adverse sequelae may be due to morphologic and functional changes in the cardiovascular system, including: • Remodeling of left ventricle • Remodeling of systemic vasculature • Development of vascular endothelial dysfunction
Hypertension Increases Risk ofCardiovascular Morbidity and Mortality The Framingham Heart Study Risk Ratio 2.2 2.5 Kannel WB Euro Heart J 1992;13(Suppl G):34-42.
Treatment Control Treatment of Hypertension Reduces Cardiovascular Morbidity and Mortality 5 Randomized Trials in 12,483 Elderly Hypertensives 494 438 438 383 346 Total Number of Individuals Affected 288 Overall BP Difference Systolic: 15 mm Hg Diastolic: 6 mm Hg % Reduction in odds: 34% p<0.001 19% p<0.05 23% p<0.001 Adapted from MacMahon S, Rodgers A. Clin Exper Hypertension 1993;15(6):967-978.
LIFE: Primary Question • In hypertensive patients at high risk of cardiovascular outcomes: • Does the mechanism of blood pressure reduction affect the magnitude of reduction of adverse cardiovascular outcomes? • Does angiotensin II receptor blockade with losartan havea greater effect on cardiovascular morbidity and mortality than conventional antihypertensive therapy when peripheral blood pressure is similarly controlled?
Losartan in Hypertensive Patients withLeft Ventricular Hypertrophy Agenda • Background and Rationale • LIFE Study Design • LIFE Patient Population • LIFE Efficacy Results • LIFE Safety Results
LIFE: Choice of Primary Endpoint • A composite cardiovascular endpoint (including cardiovascular death, stroke, and myocardial infarction) was chosen to reflect: • Systemic morbidity of hypertension on multiple organs (which may be mediated by different mechanisms) • Systemic effects of angiotensin II
LIFE: Choice of Patient Population • Hypertensive patients at increased risk of cardiovascular outcomes (including cardiac and non-cardiac events): • Left ventricular hypertrophy • Consequence of long-standing hypertension • Manifestation of systemic effects of angiotensin II • Patients likely to benefit from angiotensin II antagonism
Prevalence of LVH in the US Hypertensive Population, by Age Group NHANES III (1988-1994) Age Group
Risk of Cardiovascular Events Associated with ECG-LVH in the Elderly The Framingham Heart Study CHD Stroke Risk Ratio 3.0 3.7 3.2 5.3 Cupples LA, D’Agostino RB. NIH Publication No 87-2703, Feb 1987.
LIFE: Choice of Active Comparator • In order to answer the study question, it was necessary to utilize a comparator with: • Effective blood pressure lowering • Different primary pharmacologic mechanism • Established reduction in cardiovascular morbidity and mortality in hypertensive patients • Only -blocker- and diuretic-based regimens had proven effects on cardiovascular morbidity and mortality at the time of the initiation of LIFE study (1995)
LIFE: Choice of Active Comparator JNC V (1993) “Because diuretics and -blockers are the only classes of drugs that have been used in long-term controlled clinical trials and shown to reduce morbidity and mortality, they are recommended as first-choice agents unless they are contraindicated or unacceptable, or unless there are special indications for other agents.” Arch Intern Med 1993; 153:2413-2446.
Meta-Analysis of -Blocker Regimens in Hypertension All Cardiovascular Events † Atenolol arm. ‡ -blocker and/or diuretic arm.
LIFE: Choice of Atenolol-Based Regimen as Comparator • -blockers were known to be effective in prevention of myocardial infarction • Atenolol was effective in combination with diuretics • Atenolol had shown antihypertensive efficacy similar to losartan • Addition of diuretic to both treatment groups ensured balance in concomitant antihypertensive therapy
LIFE The Losartan Intervention For Endpoint Reduction in Hypertension Study A multicenter, multinational, double-blind, randomized, parallel study to investigate the effect of losartan, compared to atenolol, on the reduction of cardiovascular morbidity and mortality in hypertensive patients with left ventricular hypertrophy.
LIFE: Study Organization Data and SafetyMonitoring Board(Unblinded) Chair:Dr. John KjekshusUniversity of Oslo, Oslo, Norway SteeringCommittee(Blinded) Chair:Dr. Björn Dahlöf Sahlgrenska University HospitalGöteborg, Sweden Vice Chair:Dr. Richard DevereuxCornell Medical CenterNew York, NY Endpoint ClassificationCommittee(Blinded) Dr. Daniel LevyFramingham Heart StudyFramingham, MA Dr. Kristian ThygesenÅrhus University HospitalÅrhus, Denmark Merck & Co., Inc. - coordinating and data management center 945 clinical centers in 7 countries
LIFE: Hypothesis, Primary Endpoint and Secondary Component Endpoints • Hypothesis • Losartan will reduce the incidence of cardiovascular morbidity and mortality in patients with essential hypertension and left ventricular hypertrophy, as compared to atenolol • Primary endpoint • Composite of cardiovascular morbidity and mortality as adjudicated by the Endpoint Classification Committee • Secondary component endpoints • Cardiovascular mortality • Fatal and non-fatal stroke • Fatal and non-fatal myocardial infarction
Patient A 1996 1997 1998 1999 2000 2001 Dec 1995 Randomized May 1997 Non-fatal MI Feb 1999 Non-fatal stroke Sept 2000 Fatal MI Patient B 1996 1997 1998 1999 2000 2001 Feb 1997 Randomized June 1998 Fatal stroke LIFE: Primary Endpoint Analysis
Patient A 1996 1997 1998 1999 2000 2001 May 1997 Non-fatal MI Dec 1995 Randomized Feb 1999 Non-fatal stroke Sept 2000 Fatal MI Patient B 1996 1997 1998 1999 2000 2001 June 1998 Fatal stroke Feb 1997 Randomized LIFE: Primary Endpoint Analysis
LIFE: Other Endpoints Adjudicated by Endpoint Classification Committee • Total mortality (cause of death) • Hospitalization due to angina pectoris • Hospitalization due to heart failure • Coronary artery revascularizations • Peripheral revascularizations • Resuscitated cardiac arrest
LIFE: Other Endpoints • Reported by central reading laboratory • ECG: All patients (N=9193) • Left ventricular hypertrophy • Silent myocardial infarction • Echocardiography: Substudy (n=965) • Left ventricular mass index • Reported by investigator • Blood pressure • Adverse experiences • New-onset diabetes mellitus
LIFE: Disease Categories of Special Interest • Pre-specified to be of special interest: • Patients with diabetes mellitus • Patients with isolated systolic hypertension • Endpoints analyzed: • Primary endpoint • Secondary component endpoints • Total mortality • Hospitalization for angina • Hospitalization for heart failure
LIFE: Key Inclusion Criteria • Age 55-80 years • Elevated blood pressure • Systolic BP 160-200 mm Hg orDiastolic BP 95-115 mm Hg • ECG LVH • Cornell Voltage Duration ProductorSokolow-Lyon Criterion
LIFE: Key Exclusion Criteria • Secondary hypertension • MI or stroke within 6 months • Angina pectoris requiring treatment with -blocker or calcium channel antagonist • Heart failure or known left ventricular ejection fraction 40% • Conditions that required treatment with an angiotensin II receptor antagonist, -blocker, diuretic, or ACE inhibitor
LIFE: Study Design (I) Titration to target blood pressure: <140 / <90 mm Hg Losartan 100 mg + HCTZ 12.5-25 mg + others* Randomization Losartan 100 mg + HCTZ 12.5 mg Losartan 50 mg + HCTZ 12.5 mg Placebo Losartan 50 mg Atenolol 50 mg Atenolol 50 mg + HCTZ 12.5 mg Atenolol 100 mg + HCTZ 12.5 mg Atenolol 100 mg + HCTZ 12.5-25 mg + others* Day 14 Day 7 Day 1 Mth 1 Mth 2 Mth 4 Mth 6 Yr 1 Yr 1.5 Yr 2 Yr 2.5 Yr 3 Yr 3.5 Yr 4 Yr 5 * Other antihypertensives excluding ACEIs, AII antagonists, -blockers.
LIFE: Study Design (II) • Study duration: • Follow-up for minimum of 4 yearsand • Until at least 1040 patients experienced a primary cardiovascular event • Study follow-up: • Patients were to remain on study drug • Even after a study endpoint • Patients were to continue clinic visits • Even if study therapy was discontinued • Telephone contact if clinic visits not feasible • Re-start of study therapy was allowed at any time
LIFE: Endpoint Reporting and Classification • Investigators reported all potential endpoints for review by ECC • Regular monitoring visits ensured all potential endpoints reported • ECC members reviewed potential endpoints and classified independently • Differences between the initial classifications were resolved at periodic meetings • Referral to Steering Committee for resolution, if needed(no cases referred) • All potential endpoints were adjudicated (N=4363) • 21% were determined not to be endpoints • 7 with unknown cause of death
LIFE: Study Timeline 1996 1997 1998 1999 2000 2001 2002 June 1995 First patientrandomized May 1997 Last patientrandomized March 2001 Steering Committee set endpoint cut-off date(September 16, 2001) based on pooled event rate September 16, 2001 Endpoint cut-off 1096 patients with at least one primary endpoint November 2001 Final patient visit
Losartan in Hypertensive Patients withLeft Ventricular Hypertrophy Agenda • Background and Rationale • LIFE Study Design • LIFE Patient Population • LIFE Efficacy Results • LIFE Safety Results
Allocated to losartan (N=4605) Allocated to atenolol (N=4588) LIFE: Patient Disposition Entered baseline (N=10,779) Randomized (N=9222) Excluded for irregularities (n=29) Followed for study duration (N=9193) All included in ITT analyses: Complete follow-up 4500 (98%) Partial follow-up 105 (2%) All included in ITT analyses: Complete follow-up: 4496 (98%) Partial follow-up 92 (2%)
LIFE: Patient Follow-Up Atenolol (N=4588) Follow-up through death or 16-Sep-01 Patients All endpoints 4496 (98%) Partial 92 (2%) Vital status only 50 (1.0%) Withdrawn consent 34 (0.8%)Lost to follow-up 8 (0.2%) Patient-days of follow-up All endpoints 99.0% Vital status 99.4% Losartan (N=4605) Follow-up through death or 16-Sep-01 Patients All endpoints 4500 (98%) Partial 105 (2%) Vital status only 57 (1.0%) Withdrawn consent 44 (0.9%) Lost to follow-up 4 (0.1%) Patient-days of follow-up All endpoints 98.6% Vital status 99.3%
% 15.1 1.4 16.2 15.4 24.4 8.9 18.6 LIFE: Patient Recruitment N=9193 Country n 1391 133 1485 1415 2245 817 1707 Denmark Iceland Finland Norway Sweden UK USA
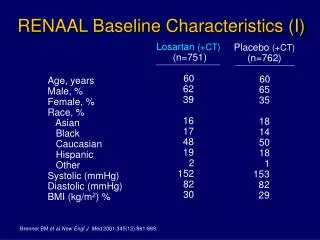
LIFE: Baseline Characteristics (I) Losartan (N=4605) Atenolol (N=4588) 66.9 54.0 92.5 5.9 1.0 0.5 0.1 66.9 54.0 92.5 5.7 1.2 0.4 0.2 Age (mean), years Gender, % female Ethnic group, % White Black Hispanic Asian Other
LIFE: Baseline Characteristics (II) Losartan (N=4605) Atenolol (N=4588) Systolic BP, mm Hg Diastolic BP, mm Hg Pulse rate, bpm BMI, kg/cm2 Smokers, % 174.3 97.9 73.9 28.0 15.8 174.5 97.7 73.7 28.0 16.8
Losartan %(N=4605) Atenolol %(N=4588) Diabetes mellitus ISH (160 / <90 mm Hg) Coronary heart diseaseMyocardial infarction Cerebrovascular diseaseStroke 12.7 14.3 16.76.7 8.24.1 13.3 14.5 15.25.7 8.04.6 LIFE: Baseline Characteristics (III) Medical History
LIFE: Baseline Characteristics (IV) Variables Utilized in Covariate Analysis ECG-LVH and Framingham Risk Score Losartan(N=4605) Atenolol(N=4588) Cornell Product, mmmsec Sokolow-Lyon, mm Framingham Risk Score, % 2828.0 30.0 22.3 2818.9 30.0 22.5 Framingham Risk Score predicts the 5-year probabilityof developing coronary heart disease based on gender, age, systolic blood pressure, smoking,total / HDL cholesterol, diabetes, ECG-LVH
LIFE: Study Therapy At Endpoint or End of Follow-Up Losartan %(N=4605) Atenolol %(N=4588) 50 mg alone 50 mg with additional drugs 100 mg with or without additional drugs Off study drug 9 18 50 23 10 20 43 27
LIFE: Study Therapy At Endpoint or End of Follow-Up Losartan %(N=4605) Atenolol %(N=4588) 50 mg alone 50 mg with additional drugsWith HCTZ onlyWith other drugs onlyWith HCTZ and other drugs 100 mg with or without additional drugsAloneWith HCTZ onlyWith other drugs onlyWith HCTZ and other drugs Off study drug 9 1814 2 2 502 18 4 26 23 10 20 14 2 4 432 16 4 22 27
LIFE: Study Therapy At Endpoint or End of Follow-Up Losartan(N=4605) Atenolol(N=4588) Time on study drug, % Mean dose of study drug, mg Time on diuretic, % Mean dose of HCTZ, mg Mean number of antihypertensive agents (including study therapy for those on drug) 86 82 72 20 2.3 82 79 70 20 2.3
Losartan in Hypertensive Patients withLeft Ventricular Hypertrophy Agenda • Background and Rationale • LIFE Study Design • LIFE Patient Population • LIFE Efficacy Results • LIFE Safety Results