Download
1 / 16
170 likes | 301 Views
Delivering VTE Prophylaxis In Acute Medicine. P Hodkinson L Renfrew P Maclean S Hannah. What are we trying to accomplish?. Aim : assess 95% of patients for VTE risk, deliver appropriate VTE prophylaxis to 95% of those patients at risk, within 24 hours of admission,

E N D
Delivering VTE Prophylaxis In Acute Medicine P Hodkinson L Renfrew P Maclean S Hannah
What are we trying to accomplish? Aim: • assess 95% of patients for VTE risk, • deliver appropriate VTE prophylaxis to 95% of those patients at risk, • within 24 hours of admission, • to the acute medical unit at Crosshouse hospital, • by October 2012.
How will we know that change is an improvement? Process: • percentage completion of risk assessment tool for VTE. • percentage completion of risk assessment tool for pharmacological thrombo-prophylaxis. • percentage delivery of thrombo-prophylactic measures to those at risk. Weekly sample for each measure of 20 randomly selected case records.
How will we know that change is an improvement? Outcome: • number of hospital associated VTE (i.e. VTE within 6 weeks of a hospital admission) • number of deaths with or caused by VTE (standardised by number of admissions or per 1000 bed days). Balancing: • adverse events caused by thromboprophylaxis. • time to assess and deliver.
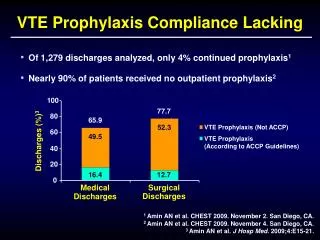
What changes can we make that will result in improvement? • Current VTE prophylaxis relies on a statement in the admission document: “Assess need for DVT prophylaxis and document whether prescribed Y/N” • No documentation of risk. • Average of 41% (30-70%) of acute medical admissions do not get VTE prophylaxis. • VTE prophylaxis has been given when it shouldn’t.
VTE prophylaxis decision tool that documents risk. A5 sized VTE prophylaxis decision tool. Medical admission document.
What changes can we make that will result in improvement? Plan: Use the tool on 1 medical admission as a printed sheet. Do: 09/01/12 – 1 doctor and I used the tool for 1 patient Study: The tool was easy to use but…the patient had ACS and therefore shouldn’t get VTE prophylaxis Act: Added a box for ACS and PE to exclude these patients.
What changes can we make that will result in improvement? Plan: Use the tool on 3 medical admissions as a printed sheet. Do: 12/01/12 – 1 doctor and I used the tool for 3 patients Study: The tool was easy to use but…it was vague around the term medical co-morbidities and it was easy to scan the bleeding risks and miss LP. Printed sheets get lost. Act: Added the full definition from SIGN 122, moved LP up the list, printed stickers.
What changes can we make that will result in improvement? Plan: Use the tool on 5 medical admissions as a sticker. Do: 23/01/12 – I put 5 stickers in 5 consecutive admission documents. I spoke to the juniors before and asked them to help. I got feedback. Study: The tool was easy to use but…dalteparin wasn’t always being prescribed or given within 24 hours. Act: Emphasized the outcome for each component of the tool.
What changes can we make that will result in improvement? Plan: Use the tool on 10 medical admissions as a sticker. Do: 14/02/12 – I put 10 stickers in 10 consecutive admission documents. I spoke to the juniors before and asked them to help. I got feedback. Study: The tool worked to document risk and dalteparin was being prescribed. Act: Get it printed in some ‘mock’ admission documents and test for a full day. Sample 10-20 from that day.
What changes can we make that will result in improvement? Plan: Use the tool as a ‘mock’ admission document for a full day. Do: 16/04/12 – LR put out 30 admission documents in ward 3E and sampled 13 of these the next day. Study: The tool is not being used. When it is used it works apart from one failure to prescribe dalteparin. Act: We need to engage medical staff in using the decision tool.
What are the challenges? • Implementing the change: • Capacity • Medical workforce • Prescribing and delivery times • Rapid turnover of patients • Senior medical resistance • Measuring: • Capacity • Outcomes – capturing hospital VTE