Download
1 / 47
470 likes | 1.01k Views
Procedure Clinic. Susana A. Alfonso, M.D. October 2, 2008 Assistant Professor Emory University Department of Family Medicine. Learning Objectives. Increase awareness of the procedures performed by Emory Family Medicine

E N D
Procedure Clinic Susana A. Alfonso, M.D. October 2, 2008 Assistant Professor Emory University Department of Family Medicine
Learning Objectives • Increase awareness of the procedures performed by Emory Family Medicine • Become familiar with the indications for colposcopy, ETST, and flexible sigmoidoscopy • Become familiar with the common complications associated with the above
Flexible Sigmoidoscopy Nasopharyngolaryngoscopy Colposcopy Circumcision Toenail excision Endometrial biopsy Splinting Exercise treadmill stress testing IUD Vasectomy Skin surgery-punch, shave, excision, I&D Joint injections Trigger point injections Procedures We Do
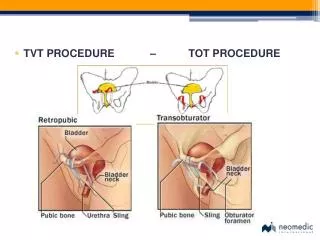
Case Number 1 28 yo female presents for a CPE with pap. She has no significant PMHx. Her Gyn Hx is as follows 13/q mo/4-5d. She is a G2P1011. She had an elective Ab following a rape in 2000. She has never had an abnormal pap or an STD. Her pap comes back ASC-US
Who gets a colpo? • ASC-US with HPV positivity for high risk types • ASC-H, LSIL, HSIL, and atypical glandular cells • Postmenopausal women and women with immunosuppression should be managed the same as the general population. This is a change • ASC-US patients who are managed with repeat cytology and show ASC-US
Contraindications • Cervicitis or severe inflammation - treat first, wait for healing. • Active bleeding or menses - wait until end of menses, if continuous bleeding colposcopy. • Significant atrophy - use vaginal estrogen cream first • Lack of an expert colposcopist -refer to someone with special training/skills
Preparation • Two advil two hours before procedure • CONSENT • Instruct patient that she will be in the lithotomy position. Saline, acetic acid and Lugol’s solution will be used and if neccessary a biopsy will be done. An ECC will complete the procedure • Use the colpo form
Remember if patient is midcycle or on hormones that the cervical mucous will be thick • Nothing in the vagina for two weeks afterward • Follow up visit to discuss results in two weeks
45 YO male with rectal bleeding intermittently for three months associated with eating hot spicy food and a “flare of hemorrhoids”. • 55 YO female without significant past medical history or family history who states she’s noticed “skinny stools”
Flexible Sigmoidoscopy: Indications • Screening of asymptomatic individuals at average risk beginning at age 50 • Screening options include : • FOBT annually • Flexible sigmoidoscopy and FOBT q 5yrs • Colonoscopy every 10 years • DCBE every 5 years
Contraindications • Family history of nonpolyposis colorectal cancer: Examine the entire colon q 1-2 years when patient is 20-30 and yearly after 40 YOA • History of adenomatous polyps • History of colorectal cancer • Ulcerative colitis • Acute peritonitis, acute diverticulitis, toxic megacolon, and recent bowel surgery
Complications • Abdominal cramping and bloating are the most common • Increased in patients who have had prior abdominal surgery • Postprocedure bleeding: usually mild and self limited secondary to trauma • Perforation: RARE one in 5,000-10,000 requires surgery
Preparation • Golytely 4Liters the night before • One oral Dulcolax the night before and two Fleets Enemas that morning • Sedatives or antispasmodics not needed • SBE prophylaxis in high risk patients
Procedure • The patient is placed in left lateral decubitus • Rectal exam • Change gloves • Insertion and visualization • Withdrawal and retroflexion • Post procedure the patient may have abdominal cramping, watery stools, or gas
Internal hemorrhoids Internal hemorrhoids with superficial necrosis
45 YO male with HTN and DM comes to you for an initial visit. He has been previously noncompliant with meds, exercise and visits but is ready to change. He denies any chest pain.
You schedule your patient for an ETST but the morning of the procedure he states that for the last two weeks since you told him to start exercising he has been feeling tight in his chest. He believes it is caused by the cold air. He remembers feeling the same way when he was a child and had asthma
Exercise Treadmill Stress Testing • Class I: Conditions for which there is evidence and/or • general agreement that a given procedure or • treatment is useful and effective. • Class II: Conditions for which there is conflicting evidence • and/or a divergence of opinion about • the usefulness/efficacy of a procedure or • treatment. • Class IIa: Weight of evidence/opinion is in • favor of usefulness/efficacy. • Class IIb: Usefulness/efficacy is less well • established by evidence/opinion. • Class III: Conditions for which there is evidence and/or • general agreement that the procedure/treatment • is not useful/effective and in some cases • may be harmful.
Indications • Class I • 1. Adult patients (including those with complete right bundle-branch block or less than 1 mm of resting ST depression) with an intermediate pretest probability of CAD (Table 4) on the basis of gender, age, and symptoms (specific exceptions are noted under Classes II and III below). • Class IIa • Patients with vasospastic angina.
Class IIb • 1. Patients with a high pretest probability of CAD by age, symptoms, and gender. • 2. Patients with a low pretest probability of CAD by age, symptoms, and gender. • 3. Patients with less than 1 mm of baseline ST depression and taking digoxin. • 4. Patients with electrocardiographic criteria for left ventricular hypertrophy (LVH) and less than 1 mm of baseline ST depression.
1. Patients with the following baseline ECG abnormalities: • Pre-excitation (Wolff-Parkinson-White) syndrome • Electronically paced ventricular rhythm • Greater than 1 mm of resting ST depression • Complete left bundle-branch block 2. Patients with documented MI or CAD Class III
Class III • Patients with severe comorbidity likely to limit life expectancy and/or candidacy for revascularization • High risk unstable angina patients
ETST and WOMEN • ST segment changes is less specific • More false positives • Less CAD • Less ability to maximally exercise…BUT • “there are currently insufficient data to justify routine stress imaging tests as the initial test for CAD in women”
Angina Typical • Defined as • 1) substernal chest pain or discomfort that is • 2) provoked by exertion or emotional stress and • 3) relieved by rest and/or nitroglycerin.
Atypical/Probable Angina Defined as chest pain or discomfort that lacks one of the three characteristics of definite or typical angina
Screening of Healthy Asymptomatic patients • Persons in high risk jobs: Pilots, mass transit operators, law enforcement, firefighters • American College of Sports Medicine recommends screening for all women over age 50 and men over age 40 who are sedentary and plan to start vigorous exercise • Persons with multiple risk factors or chronic disease
Other Indications • Evaluation of patients with known CAD after MI or after intervention • Evaluation of patients with valvular heart disease (except severe aortic stenosis) • Evaluation of exercise induced arrhythmia and response to treatment • Evaluation of rate-adaptive pacemaker setting
Absolute Contraindications • Acute myocardial infarction (within 2 d) • High-risk. Unstable angina • Uncontrolled cardiac arrhythmias causing symptoms or hemodynamic compromise • Symptomatic severe aortic stenosis • Uncontrolled symptomatic heart failure • Acute pulmonary embolus or pulmonary infarction • Acute myocarditis or pericarditis • Acute aortic dissection
Relative Contraindications • Left main coronary stenosis • Moderate stenotic valvular heart disease • Electrolyte abnormalities • Severe arterial hypertension‡ • Tachyarrhythmias or bradyarrhythmias • Hypertrophic cardiomyopathy and other forms of outflow tract obstruction • Mental or physical impairment leading to inability to exercise adequately • High-degree atrioventricular block • ‡In the absence of definitive evidence, the committee suggests systolic blood pressure of >200 mm Hg and/or diastolic blood pressure of >110 mm Hg.
Before Scheduling an ETST • Evaluate the resting EKG!!! If patients have LBBB or depressed S-T segments due to medications, electrolyte abnormalities, etc. Consider another test
Preparation • Equipment • Crash Cart • Providers trained in ACLS • NPO except water and medications • Loose fitting clothes and comfortable walking shoes • Caution with Insulin and oral hypoglycemics, digoxin, nitrates, alpha blockers, beta blockers etc.
Procedure • Pts. Undergo supine, standing and hyperventilating EKG • Bruce protocol • Increase in speed and incline q three minutes • Continuous monitoring of pts with blood pressure and pulse in the last minute of 3 minute cycle
Absolute Indications for Stopping Test • Drop in systolic blood pressure of >10 mm Hg from baseline blood pressure despite an increase in workload, when accompanied by other evidence of ischemia • Moderate to severe angina • Increasing nervous system symptoms (eg, ataxia, dizziness, or near-syncope) • Signs of poor perfusion (cyanosis or pallor) • Technical difficulties in monitoring ECG or systolic blood pressure • Subject’s desire to stop • Sustained ventricular tachycardia • ST elevation (≥1.0 mm) in leads without diagnostic Q-waves (other than V1 or aVR)
Relative Indications for Stopping Test • Drop in systolic blood pressure of (≥10 mm Hg from baseline blood pressure despite an increase in workload, in the absence of other evidence of ischemia • ST or QRS changes such as excessive ST depression (>2 mm of horizontal or downsloping ST-segment depression) or marked axis shift • Arrhythmias other than sustained ventricular tachycardia, including multifocal PVCs, triplets of PVCs, supraventricular tachycardia, heart block, or bradyarrhythmias • Fatigue, shortness of breath, wheezing, leg cramps, or claudication • Development of bundle-branch block or IVCD that cannot be distinguished from ventricular tachycardia • Increasing chest pain • Hypertensive response* *In the absence of definitive evidence, the committee suggests systolic blood pressure of >250 mm Hg and/or a diastolic blood pressure of >115 mm Hg.
Interpretation • Maximal or Submaximal: HR, METS, Double Product • Positive • Negative • Equivocal • Uninterpretable
Flexible Sigmoidoscopy Nasopharyngolaryngoscopy Colposcopy Circumcision Toenail excision Endometrial biopsy Splinting Exercise treadmill stress testing IUD Vasectomy Skin surgery-punch, shave, excision, I&D Joint injections Trigger point injections Procedures We Do
So You Want to Order a Procedure • Please precept all procedure request forms • Give them to the patient to take to scheduling • PREPARE YOURSELF • FOLLOW UP ON YOUR PROCEDURES
References • Darrow, Mark D. Ordering and Understanding the Exercise Stress Test. American Family Physician 1999;59(2): 401-414. • Johnson, Brett A. Flexible Sigmoidoscopy: Screening for Colorectal Cancer. American Family Physician 1999;59(2): 313-330. • Guidelines for the Early Detection of Colon Cancer. Reprinted from Ca-A Cancer Journal for Clinicians 2001;51(1): 44-53. • ACC/AHA 2002 Guideline Update for Exercise Testing. Journal of the American College of Cardiology http://www.americanheart.org/presenter.jhtml?identifier=3005237 (9 March 2005) • Wright, Thomas C. Jr MD et al. 2006 Concensus Guidelines for the Management of Women with abnormal cervical cancer screening tests. AJOG 2007;346-355.