Download
1 / 1
10 likes | 176 Views
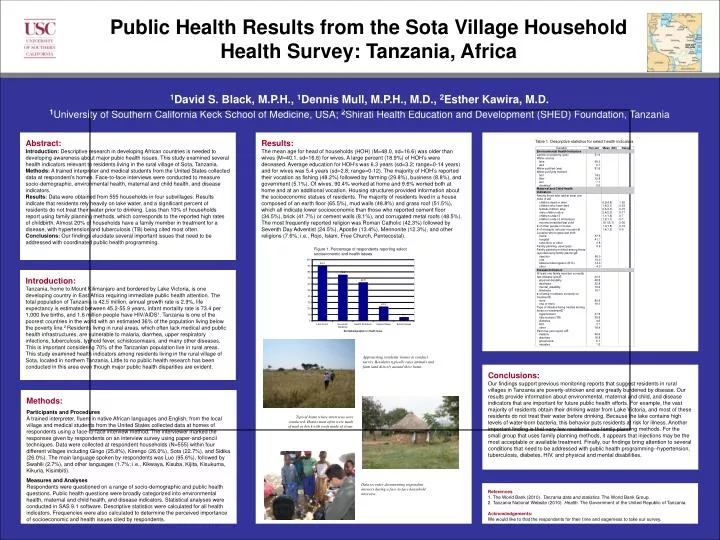
Public Health Results from the Sota Village Household Health Survey: Tanzania, Africa. 1 David S. Black, M.P.H., 1 Dennis Mull, M.P.H., M.D., 2 Esther Kawira, M.D.

E N D
Public Health Results from the Sota Village Household Health Survey: Tanzania, Africa 1David S. Black, M.P.H., 1Dennis Mull, M.P.H., M.D., 2Esther Kawira, M.D. 1University of Southern California Keck School of Medicine, USA; 2Shirati Health Education and Development (SHED) Foundation, Tanzania Abstract: Introduction:Descriptive research in developing African countries is needed to developing awareness about major pubic health issues. This study examined several health indicators relevant to residents living in the rural village of Sota, Tanzania. Methods:A trained interpreter and medical students from the United States collected data at respondent’s homes. Face-to-face interviews were conducted to measure socio-demographic, environmental health, maternal and child health, and disease indicators. Results: Data were obtained from 555 households in four subvillages. Results indicate that residents rely heavily on lake water, and a significant percent of residents do not treat their water prior to drinking. Less than 10% of households report using family planning methods, which corresponds to the reported high rates of childbirth. Almost 20% of households have a family member in treatment for a disease, with hypertension and tuberculosis (TB) being cited most often. Conclusions:Our findings elucidate several important issues that need to be addressed with coordinated public health programming. Results: The mean age for head of households (HOH) (M=48.0, sd=16.6) was older than wives (M=40.1, sd=16.6) for wives. A large percent (18.9%) of HOH’s were deceased. Average education for HOH’s was 6.3 years (sd=3.2; range=0-14 years) and for wives was 5.4 years (sd=2.8; range=0-12). The majority of HOH’s reported their vocation as fishing (48.2%) followed by farming (29.8%), business (8.8%), and government (5.1%). Of wives, 90.4% worked at home and 9.6% worked both at home and at an additional vocation. Housing structures provided information about the socioeconomic statues of residents. The majority of residents lived in a house composed of an earth floor (65.5%), mud walls (48.8%) and grass roof (51.5%), which all indicate lower socioeconomic than those who reported cement floor (34.5%), brick (41.7%) or cement walls (8.1%), and corrugated metal roofs (48.5%). The most frequently reported religion was Roman Catholic (42.3%) followed by Seventh Day Adventist (24.5%), Apostle (13.4%), Mennonite (12.3%), and other religions (7.6%; i.e., Rojo, Islam, Free Church, Pentecostal). Table 1. Descriptive statistics for select health indicators Figure 1. Percentage of respondents reporting select socioeconomic and health issues Introduction: Tanzania, home to Mount Kilimanjaro and bordered by Lake Victoria, is one developing country in East Africa requiring immediate public health attention. The total population of Tanzania is 42.5 million, annual growth rate is 2.9%, life expectancy is estimated between 45.2-55.9 years, infant mortality rate is 73.4 per 1,000 live births, and 1.6 million people have HIV/AIDS1. Tanzania is one of the poorest countries in the world with an estimated 36% of the population living below the poverty line.2 Residents living in rural areas, which often lack medical and public health infrastructures, are vulnerable to malaria, diarrhea, upper respiratory infections, tuberculosis, typhoid fever, schistosomiasis, and many other diseases. This is important considering 70% of the Tanzanian population live in rural areas. This study examined health indicators among residents living in the rural village of Sota, located in northern Tanzania. Little to no public health research has been conducted in this area even though major public health disparities are evident. Approaching residents’ homes to conduct survey. Residents typically raise animals and farm land directly around their home. Conclusions: Our findings support previous monitoring reports that suggest residents in rural villages in Tanzania are poverty-stricken and are greatly burdened by disease. Our results provide information about environmental, maternal and child, and disease indicators that are important for future public health efforts. For example, the vast majority of residents obtain their drinking water from Lake Victoria, and most of these residents do not treat their water before drinking. Because the lake contains high levels of water-born bacteria, this behavior puts residents at risk for illness. Another important finding is that very few residents use family planning methods. For the small group that uses family planning methods, it appears that injections may be the most acceptable or available treatment. Finally, our findings bring attention to several conditions that need to be addressed with public health programming--hypertension, tuberculosis, diabetes, HIV, and physical and mental disabilities. Methods: Participants and Procedures A trained interpreter, fluent in native African languages and English, from the local village and medical students from the United States collected data at homes of respondents using a face-to-face interview method. The interviewer marked the responses given by respondents on an interview survey using paper-and-pencil techniques. Data were collected at respondent households (N=555) within four different villages including Gingo (25.8%), Kirengo (26.0%), Sota (22.7%), and Sidika (26.0%). The main language spoken by respondents was Luo (95.6%), followed by Swahili (2.7%), and other languages (1.7%; i.e., Kikwaya, Kisuba, Kijita, Kisukuma, Kikuria, Kisimbiti). Measures and Analyses Respondents were questioned on a range of socio-demographic and public health questions. Public health questions were broadly categorized into environmental health, maternal and child health, and disease indicators. Statistical analyses were conducted in SAS 9.1 software. Descriptive statistics were calculated for all health indicators. Frequencies were also calculated to determine the perceived importance of socioeconomic and health issues cited by respondents. Typical home where interviews were conducted. Homes most often were made of mud or brick with roofs made of straw. Data recorder documenting respondent answers during a face-to-face household interview. References 1. The World Bank (2010). Tanzania data and statistics. The World Bank Group. 2. Tanzania National Website (2010). Health. The Government of the United Republic of Tanzania. Acknowledgements: We would like to that the respondents for their time and eagerness to take our survey.