Download
1 / 52
620 likes | 1.34k Views
Radiology Review. The following slides provide a brief overview of Radiology, including physics, image characteristics, films, processing, radiobiology and digital radiography. If you right click anywhere on the screen and select “Full Screen” the slides will be easier to view.

E N D
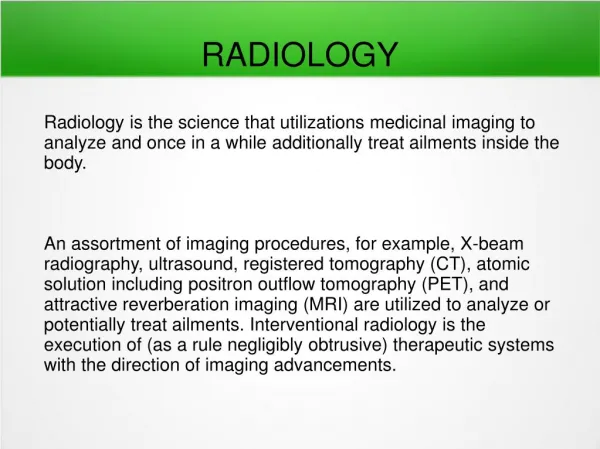
Radiology Review The following slides provide a brief overview of Radiology, including physics, image characteristics, films, processing, radiobiology and digital radiography. If you right click anywhere on the screen and select “Full Screen” the slides will be easier to view.
X-ray Machine Components kVp timer Step-up Trans. Auto PID oil filter Step-down Trans. collimator mA exposure switch The low-voltage circuit (green in diagram above) controls the heating of the filament in the x-ray tube. The mA control regulates the amount of voltage that passes through the step-down transformer, which in turn reduces the voltage to about 5 volts; this is enough to heat the filament and produce electrons.
X-ray Machine Components kVp timer Step-up Trans. Auto PID oil filter Step-down Trans. collimator mA exposure switch The high-voltage circuit (red in diagram) controls the voltage across the x-ray tube. It is regulated by the kVp selector (a rheostat) and the step-up transformer, resulting in a very high voltage which pulls the electrons from the filament to the target. The higher the kVp, the greater the energy of the electrons
X-ray Tube molybdenum focusing cup tungsten filament electron flow tungsten target copper sleeve unleaded glass window leaded glass vacuum inside tube electrical connections x-ray When the exposure switch is depressed, the filament is heated, producing a cloud of electrons around the filament. The high voltage between the cathode (filament, focusing cup) and the anode (target, copper stem) pulls the electrons across the x-ray tube to interact with the target to produce x-rays.
Bremsstrahlung X-ray Production high-speed electron x-ray + decelerated electron The majority of x-rays produced are known as Bremsstrahlung. These x-rays result from the attraction between the high-speed electrons (negative charge) from the filament and the protons (positive charge) in the nuclei of the target atoms. The attraction causes the electron to slow down and change direction, resulting in the release of energy in the form of an x-ray. The closer the electron passes to the nucleus, the greater the energy of the resultant x-ray. If the electron hits the nucleus, a maximum energy x-ray results.
60-cycle Alternating Current Constant Potential (800 cycles.sec.) With alternating current, x-rays are only produced during the positive half of the cycle (red areas above). There is a large fluctuation in the voltage between the filament and the target, contributing to a wide range of x-ray energies. X-ray machines with constant potential (“direct current”) are preferred over the standard alternating current. This provides more efficient x-ray production and less exposure time per radiograph. Most of the newer x-ray machines utilize constant potential.
kVp determines the voltage across the x-ray tube. This ultimately determines the energy (penetrating ability) of the x-ray beam. Higher kVp = higher average energy (dotted lines above) and higher maximum energy. There is also an increase in the number of x-rays produced when kVp is increased. Increasing the kVp allows you to reduce exposure time (An increase of 15 kVp allows you to cut the exposure time in half). It is recommended that at least one x-ray machine in the office have the capability of varying the kVp (to image children, patients with tremors, etc., which requires minimum exposure time). In general, a higher kVp is preferred, especially for periapical and periodontal diagnosis.
An increase in the mA setting or the exposure time results in an increase in the number of x-rays produced. There is no change in the average energy of the x-ray beam. A machine with variable mA settings would normally be set at the highest mA, allowing for a reduced exposure time. Exposure time: 60 impulses = 1 sec.
Density = degree of darkening. Affected by: Exposure factors (Increase = increase in density) Size of head (soft tissue, bone): Increase will result in decrease in film density Object density (bone, teeth, restorations): Increase will result in decrease in film density Film fog (scatter, storage): Results in increase in overall film density Contrast = density differences. Increased by: Lowering kVp An increase in subject contrast Technically, higher contrast (lower kVp) is preferred for caries detection. Lower contrast (higher kVp) is recommended for imaging periapical and periodontal changes. For general use, a medium kVp (70-75) is usually selected.
Sharpness Measures how well the details (boundaries) of an object are reproduced on a radiograph Increased by: Source-object distance Object-film distance Film crystal size Motion will decrease sharpness Magnification Decreased by: Source-object distance Object-film distance
16” FFD image Target 16” from film Target 8” from film 8” FFD image Film Increasing the distance from the target of the x-ray tube (focal spot, focus) to the object (teeth/film) (FFD = focus-film distance) will result in an increase in sharpness and a decrease in magnification. This results when a longer PID (cone) is used. Moving the film closer to the teeth will also increase sharpness and decrease magnification.
8" FFD 12" FFD Most newer x-ray machines have a recessed target (away from the PID). This helps to increase the focus-film distance (FFD), resulting in a sharper image and less magnification without an increase in the length of the PID (position indicating device). A longer PID is effective, but it makes positioning the tubehead more difficult.
Intraoral Film D-speed (Ultraspeed):Probably the most commonly used film in private practice. Technically will give you sharper image, because of the smaller crystal size. F-speed (Insight): Larger silver halide crystals. 60% less radiation than D-speed.
Clinasept Barriers (see above) seal the film inside plastic, protecting the film from saliva. When the films are separated out of the plastic, the films can be handled for processing with minimal risk of contamination. The cost for the film/barrier combination is more expensive than film alone, but the advantages in infection control are obvious.
Extraoral film for panoramic or cephalometric radiographs comes in various types/sizes. T-Mat film is available as G (high contrast), L (wide latitude) and H (used when taking two films at same time to provide extra film). In general, T-Mat L film is used because exposure factors are not as critical for slight variations in patient size (wider latitude). These films are used with rare earth screens (emit green light). Ektavision screen/film combinations are also available (G, H, L films). This system produces images with more detail than the T-Mat system (same speed). Ektavision screens also emit green light.
Intensifying Screens Calcium Tungstate Barium Strontium Sulfate Rare Earth Lanex (used with T-Mat film) Ektavision speed Intensifying screens for panoramic or cephalometric imaging should be a type of rare earth screen (green-light emitting). These screens require less radiation exposure (than blue light emitting) with no loss of image detail. Patient exposure is reduced.
Film Viewing Guidelines Mask viewbox (block light around film mount) No distractions View films when alert, refreshed (not at the end of the day) Use magnifying lens Vary illumination of viewbox if possible (rheostat) Reduce room light
Radiobiology Some patients are very concerned about the amount of exposure they are getting from a series of radiographs. It is important to understand the effects of x-rays and what the approximate doses are from individual films. The following slides briefly describe the effects and doses associated with routine radiographic procedures.
When x-rays enter the body, they interact with the atoms of the various tissues, causing ionization (removal of an electron from the atom). This results in the formation of ions and free radicals which are very reactive and join with other atoms/molecules to form undesirable combinations (mutations). If the x-ray interacts with a critical molecule, especially DNA, the molecule’s chemical bonds are broken and this may alter the function of the DNA and ultimately the cellular activity. This is the direct effect of radiation. If the x-ray interacts with another, non-critical molecule (usually water), the ions and free radicals produced may in turn interact with a critical molecule and cause damage. This is the indirect effect.
Permanent damage Dose According to the LNTH (Linear No-Threshold Hypothesis; blue line above) any dose, no matter how small, will result in some permanent damage within the cells affected. New molecular and cellular biology data demonstrate that cellular control of massive natural DNA damage rates contradicts the biological plausibility of the LNTH; in other words, cellular repair takes care of any damage below a certain dose. This is represented by the red line above.
It has been estimated that 8,000 to 10,000 DNA-damaging events occur spontaneously in each cell every hour. This damage is successfully repaired within minutes of its occurrence. 1 cGy (1 rad) of radiation produces 80 DNA damage sites. It is felt that if the cells can successfully repair the damage from 8,000-10,000 spontaneous events, the 80 (1 %) more from x-ray exposure would also be repaired.
Radiation Effects influenced by: Total Dose: Higher dose = greater effect Dose Rate (all at once = greater effect or spread over a period of time = less damage) Area covered (volume of tissue): more tissue = greater effect Type of tissue (radiosensitive = greater effect, radioresistant = reduced effect) Age: greater effects in young people
Background Radiation = 360 mrem/year Radon 200 mrem (54%) Cosmic (sun) 27 mrem (8%) Rocks/soil 28 mrem (8%) Internal 40 mrem (11%) Medical x-rays* 39 mrem (11%) Nuclear medicine 14 mrem (4%) Consumer products 10 mrem (3%) Other sources < 1 mrem (1%) * Dental x-rays 0.1% Everyone is exposed to certain amounts of background radiation; the amount will vary depending on where you live, the amount of outdoor activity, etc.. Radon is by far the largest contributor to the background total and the radon levels in your house should be checked. Dental x-rays contribute a very small portion to the background total.
Surface X-ray Exposure Periapical/BW: 100 mR (F-speed) 250 mR (D-speed) Panoramic: 500 mR AFM: 2.0 R* (F-speed) Lateral Skull: 200 mR Chest: 20-40 mR *1 R = 1000 mR These numbers will vary depending on the source of the information, but they are in the ballpark. Keep in mind that these numbers don’t take into account the total area covered; the next slide gives a more accurate indication of the total exposure a person receives.
Effective Dose AFM (round, F-speed) 6.7 mrem AFM (rect., F-speed) 2.6 mrem Panoramic 0.7 mrem Skull 22.0 mrem Chest 8.0 mrem Effective dose is the approximate whole-body dose received from the various x-ray procedures. A full series of intraoral films, with round collimation and F-speed film, results in less exposure than a chest film, which uses intensifying screens and is looking at soft tissue.
MPD Maximum Permissible Dose The MPD represents the amount of radiation an individual is allowed to receive from artificial sources (such as x-ray machines). The values listed below are per year. Occupationally exposed 50 mSv (5 rem) NCRP* General Population 5 mSv (.5 rem) NCRP *National Council on Radiation Protection
The exposure a patient receives from a full-mouth series of x-ray films is approximately the same as the exposure received while traveling from New York to LA on a plane. (Using F-speed film). One-in one million chance of dying: Obviously, we don’t want to mention dying in connection with x-rays, but it puts things into perspective regarding the effects/risks of taking radiographs. AFM Smoking 1 cigarette Riding a bicycle 10 miles Driving a car 300 miles Flying 1000 miles
Patient Protection Film ordering (Risk vs. Benefit) Equipment reliability Filtration Collimation Film/screen speed Lead apron/thyroid collar Technique Processing
Ordering Films Clinical exam – should be done before deciding what films are needed. Selection Criteria – developed by ADA and other groups; these serve as guides in deciding what films are necessary. (See next slide). Professional Judgment – based on clinical experience, didactic training, etc.
Selection Criteria Symptomatic teeth Fracture/chipped tooth Large caries Large restorations Abutment teeth Gingival condition Selection criteria are used to identify teeth which are potentially at risk (or are to be used as abutments) and require periapical films to identify periapical changes.
Equipment Reliability Leakage Radiation Timer Accuracy X-ray production (kVp, mA) State Inspection by Ohio Department of Health X-ray machines are required to be inspected every five years in Ohio. If you take over an existing practice, I recommend that you contact the ODH to schedule an inspection if one has not been done recently.
Filtration Aluminum filter(s) Added 2.5 mm Total 70 kVp Glass window of x-ray tube Oil/metal barrier 1.5 mm Inherent The amount of filtration is regulated by the government (NCRP). Any machine capable of operating at a kVp of 70 or above must have 2.5 mm aluminum equivalent of total filtration. If the maximum kVp of the machine is 65, only 1.5 mm aluminum equivalent is needed. The manufacturer automatically provides this on x-ray machines.
Collimation controls the size of the x-ray beam. Allowed beam size is a maximum of 2.75 inches (7 cm) in diameter at skin surface. 7 cm If you switch from a 7 cm round PID to a 6 cm round PID, the patient receives 25% less radiation. Switching from 7cm round PID to rectangular PID reduces dose by 55%. 6 cm 7 cm round 6 cm round # 2 film (4.5 cm long) entrance entrance exit exit
Lead Apron/ Thyroid Collar Some people are suggesting that lead aprons are not needed. However, most feel that any reduction in patient exposure is beneficial and, since the cost and time of placement of the apron are minimal, the use of the apron is encouraged. I recommend a lead apron with a separate, but attached, thyroid collar for intraoral films. For panoramic or ceph films, a double-sided apron with no collar is used. There are multiple sources for lead aprons.
Pregnancy ….the fetal exposure is only about 1 microGray for a full-mouth series. Accordingly, the guidelines for ordering films can be used with pregnant patients just as with other patients. The unborn child is very sensitive to ionizing radiation. Limit radiographic examination during pregnancy to cases with a specific diagnostic indication. Postpone elective procedures until the termination of the pregnancy. The apparently contradictory views above came from the same textbook. Bottom line: Do what you think is best for your pregnant patient.
X-ray Protection for the Operator • Do not hold films for patient • Utilize barriers if possible Door with leaded glass Wall of room (drywall adequate protection); need mirror mounted opposite doorway so that you can see patient in operatory • Adhere to position-and-distance rule if no barriers available (see next slide)
Position and Distance Rule 135° 135° 6 feet 6 feet 90° 90° If no barriers are available, you should stand at least six feet away from the patient at an angle of 90-135 degrees to the direction of the x-ray beam, on either side of the patient (footprints in diagram above).
Film badges are only required if you expect to exceed 10% of the MPD (0.05 Sv or 5 rem) during the year. Since you should not exceed this amount if you follow routine radiation protection procedures, film badges are not required in the State of Ohio. However, I feel it is a good idea to provide badges for your assistants/hygienist for their peace of mind, at least for a 3-month period. If no exposure is recorded during that time, it is unlikely that any future exposure will occur and the badges can be discontinued.
Ohio Department of Health Radiologic Health Program Registration For purchase, transfer, or disposal of x-ray equipment Biennial registration fee Inspection Every five years (private practice) Inspection fee per machine
State Requirements Radiation Safety Officer (Dentist, hygienist, or assistant) Notice to Employees (Must be prominently displayed); available from state. Safe Operating Procedures (List of x-ray machines, settings, usage, etc.) Instruction of Individuals (Signed form indicating employee familiar with x-ray procedures) Contact the Ohio Department of Health, Radiologic Technology section for information and guidelines to satisfy above requirements. (614) 752-4319.
Ohio State Dental Board (614) 466-2580 Assistants need Radiographer’s license to take radiographs. Need 7 hours of CE followed by in-office training. Two hours of radiology CE then required every two years.
Digital Radiography Advantages Reduced patient exposure (Intraoral) Ability to manipulate image Patient consultation/education “Instant” image (CCD, CMOS) No chemical processing Environmentally friendly (no processing chemicals, silver, lead) Remote consultation Lower long-term cost?
Digital Radiography Components X-ray machine: Standard intraoral or pan/ceph machine Sensor (CCD, CMOS, PSP; see next slide) Laser scanner (PSP only) Computer with monitor and modem or high-speed cable connection Printer
Direct Digital (Sensor connected directly to computer) CCD: Charged Coupled Device CMOS: Complimentary Metal Oxide Semiconductor Indirect Digital (Requires laser scan of sensor) PSP: Photo-Stimulable Phosphor
sensor PSP plastic sleeve* sensor * Protects film from saliva CCD, CMOS to computer covered with plastic sleeve and finger cot before placing in mouth
CCD, CMOS These digital sensors are composed of a pure silicon chip divided into an array of pixels (picture elements). When x-rays strike the surface of the sensor, energy is stored in the pixel; the amount of energy stored is determined by the strength of the x-ray hitting a particular pixel. These charges are then removed electronically, in sequence, creating an output signal with a voltage proportional to the energy stored in each pixel. These signals produce the digital image seen on the monitor.
PSP (Photostimulable phosphor) These phosphors absorb x-ray energy in a manner similar to the phosphors used in intensifying screens. X-rays striking the phosphor excites electrons in the atoms, some of which produce light but the majority of which are trapped within the phosphor. When the sensor is scanned with a ruby laser, the trapped electrons are released, causing emission of shorter-wavelength light in the blue region of the spectrum. The more x-rays absorbed by the phosphor, the brighter the light. The emitted light is detected by a photomultiplier tube and the information is digitized to form the image.
CCD and CMOS systems produce an “instant” image and can be useful for endo or emergencies. The sensor is very thick and rigid and can be more difficult to place in the mouth. The sensors cost several thousand dollars to purchase or replace. Pan/ceph systems are much more expensive.
PSP systems require laser scanning of the sensors which takes several minutes (time to load films in scanner and scan). Sensors are actually thinner than x-ray film and are more comfortable for the patient. Intraoral sensors cost about $35; you would need to have enough sensors for at least two full series in order to function effectively. Pan/ceph sensors cost around $800-900. The initial cost of the PSP system is higher than CCD or CMOS systems because of the cost of the laser scanner. (This assumes you only have one CCD/CMOS sensor).
Schick has developed a wireless sensor that will produce an “instant” image as do the corded sensors. However, the wireless sensor is much thicker and more expensive. Several systems use laptop style computers for imaging. This allows easy portability between operatories. The old-style CRT monitors will give you better x-ray images, but many feel the overall space-saving and great color for intraoral pictures make flat-panel monitors the best choice in the operatory.