Download
1 / 17
170 likes | 353 Views
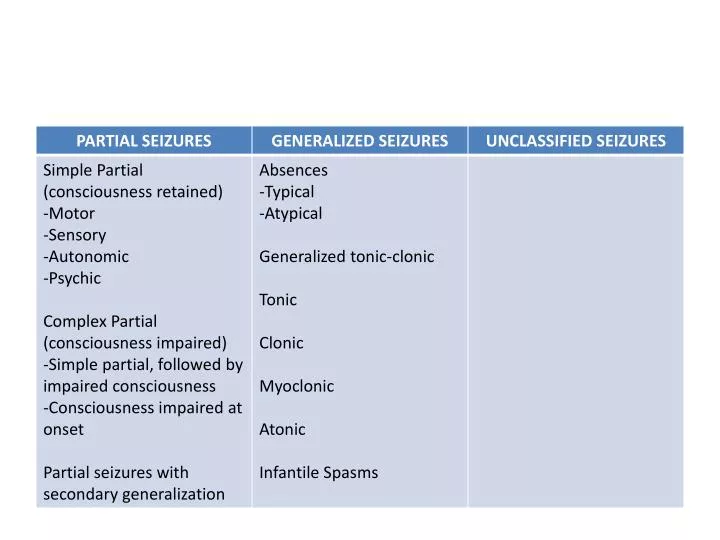
SIMPLE PARTIAL SEIZURES (SPS). Motor activity – most common symptom Asynchronus clonic or tonic movements Tend to involve the face, neck, and extremities Some patients complain of aura Lasts for 10-20 secs Patients remain conscious and may verbalize during seizure

E N D
SIMPLE PARTIAL SEIZURES (SPS) • Motor activity – most common symptom • Asynchronusclonic or tonic movements • Tend to involve the face, neck, and extremities • Some patients complain of aura • Lasts for 10-20 secs • Patients remain conscious and may verbalize during seizure • No postictal phenomenon
May be confused with tics (shoulder shrugging, eye blinking, and facial grimacing and primarily involve the face and shoulders; can be briefly suppressed, but SPS cannot be controlled) • EEG- spikes or sharp waves unilaterally or bilaterally or a multifocal spike pattern
COMPLEX PARTIAL SEIZURES (CPS) • May begin with a SPS with or without an aura, followed by impaired consciousness • Aura- vague, unpleasant feeling, epigastric discomfort, or fear – 1/3 of children with SPS or CPS; indicates focal onset • AUTOMATISMS- common feature of CPS in infants and children occurring in about 50-75% of cases • Alimentary automatisms in infants: lip smacking, chewing, swallowing, and excessive salivation • In children: semi-purposeful, incoordinated, unplanned automatisms
PARTIAL SEIZURES WITH SECONDARY GENERALIZATION • Secondary generalization – spreading of the epileptiform discharge • Contralateralversive turning of the head, dystonic posturing, and tonic-clonic movements of the extremities and face, including eye blinking • 1-2 mins • EEG- anterior temporal lobe sharp waves or focal spikes and multifocal spikes
ABSENCE SEIZURES • Sudden cessation of motor activity or speech with a blank facial expression or flickering of the eyelids • More prevalent in girls before 5 years old • Never associated with an aure • Rarely persists longer than 30 secs • Not associated with a postictal state • EEG- 3/sec spike and generalized wave discharge • COMPLEX ABSENCE – myoclonic movement of the face, fingers, or extremities, loss of body tone; EEG – atypical spike and wave discharges 2-2.5/sec
GENERALIZED TONIC-CLONIC SEIZURES • Common and may follow a partial seizure with a focal onset • Maybe associated with an aura • Patients suddenly lose consciousness, eyes roll back, and body musculature undergoes tonic contractions, become cyanotic • Clonic phase – rhythmic clonic contractions alternating with relaxation of all muscle groups • Loss of sphincter controll, particularly the bladder
Postictally, children are initially semicomatose and typically remain in deep sleep for 30 mins to 2 hrs
MYOCLONIC EPILEPSIES OF CHILDHOOD • Repetitive seizures consisting of brief, often symmetric muscular contractions with loss of body tone and falling or slumping forward • BENIGN MYOCLONUS OF INFANCY • TYPICAL MYOCLONIC EPILEPSY OF EARLY CHILDHOOD • COMPLEX MYOCLONIC EPILEPSIES • JUVENILE MYOCLONIC EPILEPSY (Janz Syndrome) • PROGRESSIVE MYOCLONIC EPILEPSIES
INFANTILE SPASMS • 4-8 months • Brief symmetric contractions of the neck, trunk, and extremities • 3 types: flexor, extensor, and mixed • FLEXOR: occur in clusters or volleys and consist of sudden flexion of the neck, arms, and legs onto the trunk • EXTENSOR: extension of the trunk and extremities; least common • MIXED: flexion in some volleys and extension in others; most common • EEG- hypsarrhthmia-chaotic pattern of high voltage, bilaterally asynchronous, slow-wave activity or a modified hypsarrhythmia pattern
Cryptogenic or Symptomatic • CRYPTOGENIC: uneventful pregnancy and birth history as well as normal developmental milestones before onset of seizures • SYMPTOMATIC: prenatal, perinatal, and postnatal risk factors
NEONATAL SEIZURES • FOCAL – rhythmic twitching or muscle groups, particularly those of the extremities and face • often associated with localized structural lesions as well as with infections and subarachnoid hemorrhage • MULTIFOCAL CLONIC- similar to focal clonic but differ in that many muscle groups are involved, frequently several simultaneously
TONIC- rigid posturing of the extremities and trunk, sometimes associated with fixed deviation of the eyes • MYOCLONIC- brief focal or generalized jerks of the extremities or body that tend to involve distal muscle groups • SUBTLE- chewing motions, excessive salivation, and alterations in then respiratory rate including apnea, blinking, nystagmus, bicycling or pedaling movements, and changes in color
EEG CLASSIFICATION OF NEONATAL SEIZURES • CLINICAL SEIZURE WITH A CONSISTENT EEG EVENT • CLINICAL SEIZURES WITH INCONSISTENT EEG EVENTS • ELECTRICAL SEIZURES WITH ABSENT CLINICAL SEIZURES
CLINICAL SEIZURE WITH A CONSISTENT EEG EVENT • Clinical seizure occurs in relationship to seizure activity recorded on EEG • Includes focal clonic, focal tonic, and some myoclonic seizures • Epileptic and are like to respond to anticonvulsants
CLINICAL SEIZURES WITH INCONSISTENT EEG EVENTS • Observed with all generalized tonic seizures and subtle seziures and with some myoclonic seizures • Infants tend to be neurologically depressed or comatose as a result of hypoxic-ischemic encephalopathy • Nonepileptic origin • May not require or respond to antiepileptics
ELECTRICAL SEIZURES WITH ABSENT CLINICAL SEIZURES • May develop in comatose infants who are not on anticonvulsants • May persist in patients with focal tonic or clonic seizures without clinical signs after the introduction of an anticonvulsant