Download
1 / 24
240 likes | 368 Views
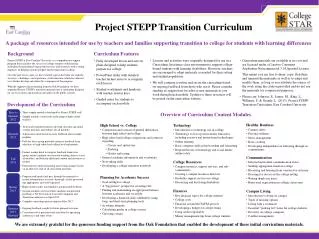
GHC Transition Project. Youth Health Transition Initiative Ann Behrmann, MD Mala Mathur, MD, MPH February 10, 2014. History of Pediatric Medical Home Pilot Projects at GHC 2004-2014.

E N D
GHC Transition Project Youth Health Transition Initiative Ann Behrmann, MD Mala Mathur, MD, MPH February 10, 2014
History of Pediatric Medical Home Pilot Projects at GHC 2004-2014 • Comprehensive Care Plans (CCP) in EMR: Office Workflows to develop and update CCP with original medical home team (care management RN, team RN, MD, parent advocate, Waisman Southern Regional Center for CYSHCN) • Developmental Screening Project—incorporated ASQ, into all 9,18,24 and 36 mo WCC and MCHAT into visits with tracking • Kids Medical Home website (http://duff-co.com/KMH) • Transitions Project
Why a transitions project? • Primary Care transitions from pediatric to adult care are happening but currently there is no organized procedure resulting in a lack of parent/patient education about this process. • Healthy People 2020 includes improving the healthy development, health, safety, and well-being of adolescents and young adults. • New NCQA requirements include components of transition process from pediatric to adult healthcare
GHC Transition Project 2012-2014 • Worked closely with national partners “Got Transition” and with state partners “Wisconsin Youth Health Transition Initiative” to understand latest guidelines and to get support with already developed resources/tools. • Done as an ABP MOC project (25 credits) with Got Transition team and WI state partners • Pilot Project using Transition Checklists Fall 2012-Summer 2013 • Presented findings from GHC’s Pilot Project at “14th Conference on Disability and Chronic Illness: Transition from Pediatric to Adult based Care” at Baylor October 2013
Pilot Project Fall 2012-Summer 2013 • Developed Policy Statement on Transition for our organization • Gave out Transition Checklist to all adolescents age 12-22—at both sick and well visits • Used Checklist as a springboard for discussion about the transition process • Initiated separate transition visits for a handful of our YSCHN • Worked on developing patient education materials for teens and parents • Worked on Smart Text (and specific AVS info) for transition
Methods • Checklists given to all youth (healthy and YSHCN) age 14-22 for both well and acute care visits over a 14 month period (July 2012-September 2013) • YSCHN defined in this study as youth with chronic medical conditions that impact their functioning and require care above a typical healthy adolescent • Checklists given to parent if present with youth for office visit Total number of youth participants = 92 Total number of family participants = 63
Results of Pilot Project • Transition Checklists were confusing as kids of all ages were given the same checklist and verbiage was unclear at times • Most families were very interested in finding out what they could do to help prepare their child for the changes they face when accessing health care as an adult • Patient education materials were needed to help support what verbal patient education was being given by provider • Realized need to involve multiple GHCSCW departments: Quality Improvement , Information Technology, Compliance Officers, Marketing, Nursing Supervisor in process development
Tangibles from Transition Work • Revised Checklists that are broken down by age group (age 12-14, age 15-17, age 18 and up) • “Tool Kit for Teens”-patient educational handout • “Health Care Transition in Adolescence”- parent educational handout • Transitions Policy and Procedure for GHC (draft) • Transition Introductory Letter to parents (draft)
Policy to Procedure • Need to develop workflow procedure for CNA, LPN, RN, Provider—this being done by our team RN and Care Management RNs • For separate transition visits for YSHCN, need to consider pre-visit prep: possibly as 30 min RN/30 min provider visits or other supported workflow • Can code for transition work (phone care coordination and visits)
Barriers to Workflow • Education for providers/staff about importance of transition • Need to develop Patient Registry for Transition in YSHCN population in EMR which is accessible and editable • Time for RN to do pre-visit prep and for provider to update CCP and problem list regularly at least every 6 months(problem based charting may help in future)
Barriers to Workflow Continued… • Time constraints for developing good communication between pediatric MD and FP or IM provider who will assume care of young adult • Time constraints for joint visits with patient and both MDs (peds and adult provider) to review problem list, medications, PE issues • Incorporating Care Management, Social Work, Behavioral Health into Transition Process • EMR: Working on getting checklists into flow sheet and adding patient education materials to AVS and possible BPA to help populate problem list (allow for outcome measurements)
Transition and EPIC • Currently: • Smart Set with Smart Text on transition drafted in 2013 • Future: • Working on getting patient education materials in AVS • Working on flow sheet for checklist • Working on Best Practice Alert • Working on adding smart data elements to a newly inserted question in WCC (12-17 year) to track how many members are getting transition education and develop outcome measures to evaluate transition process –looking at both sustaining quality of care and patient, staff satisfaction
Challenges for Transition • MyChart- need way to have confidential communication with both adolescents and parents • Full functionality of MyChart for families of YSHCN between ages 12-17 years within HIPAA guidelines • Identification of adult providers at GHC who will accept YSHCN • Developing a process for joint visits with YSHCN and peds and adult MDs • Coordinated transition of UW specialty care from Pediatric to Adult Services (for some specialties considering teen/young adult clinics that focus on self care, prevention, understanding of health issues)
Next Steps continued • Share process with colleagues to help support all families at GHC in the transition process • Training of staff to use checklists and providers to utilize smart sets and AVS resources • Build and utilize means to evaluate Transition process and outcome measures to monitor usefulness to patients, GHCSCW
TRANSITIONS: From a Family Medicine Perspective Leah Ederer, MD
Difficulties • No clear transition time • Because of family setting we are often seeing parents as patients as well who ask questions about their children or speak for their children • MyChartdifficulties • Messages in parents chart not “kidschart” • Parents creating children’s e-mails
College Students • University Health Services • Involved in the student community • Available for help with projects • Facebook and Twitter • Easy to navigate and informative website http://www.uhs.wisc.edu/ • New student checklist including immunizations needed
http://www.uhs.wisc.edu/about-uhs/documents/entranceletter.pdfhttp://www.uhs.wisc.edu/about-uhs/documents/entranceletter.pdf
College Students • Location issues • On parents insurance • Can only be seen over break • MyChart and refills over a distance • Mental Health Issues • Back and upper extremity injuries from computer use
Implementation • Split appointment • 30 min with RN for checklist and education • 30 min with MD for questions and physical • Similar structure already successful with pre-op and Medicare physicals. • Checklist format already available for OB visits