Download
1 / 63
640 likes | 1k Views
VTS PATIENT SAFETY TRAINING DAY Dr Christine Johnson, National Patient Safety Agency Dr Jane Carthey, Human Factors Specialist, JCC. Objectives of the day. To update you on the field of patient safety To explore patient safety issues in primary care

E N D
VTS PATIENT SAFETY TRAINING DAYDr Christine Johnson, National Patient Safety AgencyDr Jane Carthey, Human Factors Specialist, JCC
Objectives of the day • To update you on the field of patient safety • To explore patient safety issues in primary care • Introduce you to the work of national agencies who have a role in improving patient safety • To encourage you to consider how this work applies to your practice.
Today’s Agenda • 09.30- 09.40am Introduction and purpose • 09.40-10.25am Patient Safety for GPs: What are the issues? • 10.25-10.40am Patient safety in Primary care: Setting the Scene • 10.40-11.00am Coffee Break • 11.00-12pm Patient Safety Research: A GP’s personal perspective • (Professor Aneez Esmail) • 12-12.30pm E-learning demonstration • 12.30-1.15pm Lunch • 1.15-2.15pm Prescribing oral anti-coagulants safely • 2.15-3.30pm Being open • 3.30-4.00pm Feedback and evaluation of the day
Format of the day • Mixture of presentations and group work • Aims to be interactive and discursive • E-learning material • Video and forum theatre based Being open session
Patient Safety for GPs: What are the issues? Dr Christine Johnson, National Patient Safety AgencyDr Jane Carthey, Human Factors Specialist, JCC
Patient Safety for GPs: What are the issues? • Work in groups at your table • Introduce yourselves to each other • Identify the patient safety issues that occur in a GP Practice. • Types of patient safety incidents you have experienced or heard about through local incident reporting or discussions with colleagues. • Capture your responses on flip chart paper • 30 minutes group discussion • 15 minute feedback session
Patient Safety In Primary Care: Setting the Scene Dr Jane Carthey
Patient Safety In Primary Care: Setting the Scene • Types of errors and incidents in primary care • National agencies with a role in improving patient safety
Errors during GP consultations • Sandars and Esmail (2003) reviewed eleven studies relating to medical error in primary care to identify the frequency andnature of errors. • Overall, the studies reported wide differences in rates of errorsin primary care, varying from five to 80 per 100 000 consultations.
Errors during GP consultations • Diagnostic errors were consistently the most frequent incident type across all studies, varying from 26 to78% of identified errors. • Both delayed and missed diagnoses were identified as the error type most likely to result in major harm. • The second most common category of errortype related to treatment, either delayed or inappropriate,varying from 11 to 42% of identified errors. • These errors wereless likely to result in major harm to the patient.
Errors in GP practices • UK study using an anonymous self-reporting system to identify errors occurring in the GP practices in the North East of England • Two week data collection period 940 errors were recorded from 10 practices 42% (397/940) were related to prescriptions, although only 6% (22/397) of these were medication errors. • Communication errors accounted for 30% (282/940) of errors and clinical errors 3% (24/940). • The overall error rate was 75.6/1000 appointments (95% CI 71 to 80) (Rubin, George et al., 2003).
Prescribing errors • Incorrect drug, dose, frequency, drug interactions etc.. • Avery et al., (2005); GPs expectations and beliefs about electronic prescribing systems • Many GPs were unsure as to whether the system they were currently using possessed key features. • Some GPs erroneously believed that their computers would warn them about potential contraindications or if an abnormal dose frequency had been prescribed. • Only a minority had received formal training on the use of their system's patient safety features
National agencies • National Patient Safety Agency • NICE • Royal Colleges (including RCGP) • National Institute for Innovation and Improvement • Healthcare Commission • NHSLA Plus many others…
National Patient Safety Agency • Collect and analyse information on patient safety incidents in the NHS • Assimilate other safety related information from within the UK and worldwide • Learn lessons and ensure that they are fed back into practice • Where risks are identified - produce solutions to prevent harm, specify national goals, establish mechanisms to track progress • Building a safer NHS for patients • Department of Health (2001)
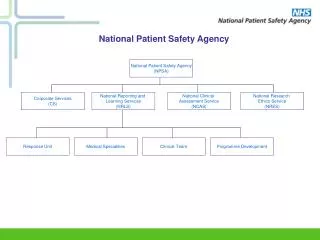
National Reporting & Learning System (NRLS) Feedback International Collaboration Australia USA Europe Standardised reporting NPSA NHS Trusts PractitionersStaff Healthcare Commission MHRA NHS Complaints NHS Litigation Authority Patients Carers
Reason’s Swiss cheese model Levels of defence LATENT CONDITIONS: poor design, procedures, management decisions etc.. Patient Safety Incident ACTIVE ERRORS
Patient Safety Research: A GP’s Personal Perspective Professor Aneez Esmail, Professor of General Practice, School of Medicine. University of Manchester
E-learning introduction and demonstration Alan Mullen, E-learning advisor Adam Crowley, E-learning advisor E- Learning for Health
Prescribing oral anti-coagulants safely Dr Jane Carthey & Dr Christine Johnson
Safe Medication Practice Work Programme 2007 - 2008 • Five Patient Safety Alerts on High Risk Issues: • Actions that can make the use of anticoagulants safer • Promoting safer measurement and administration of oral liquid medicines • Promoting safer practice with injectable medicines • Safer practice with epidural injections and infusions • Reducing the risk of hyponatraemia when administering intravenous infusions to children • Work led by Professor David Cousins at the NPSA
UnderstandingAnticoagulant Incidents • The NPSA contacted the medical and pharmacy defence organisations as well as the NHS Litigation Authority. • There have been 480 reported cases of harm or near harm from the use of anticoagulants in the UK from 1990-2002. • In addition there have been 120 deaths reported over the same time period. • Deaths from the use of warfarin is responsible for 77% (92 reports) and heparin is responsible 23% (28 reports).
The 3-bucket model forassessing risky situations (Reason, 2005) 3 2 1 Self Context Task
Warfarin incident scenario 1 • Read through first page of the scenario ONLY! • In your groups, discuss what went wrong • Think about the Three Buckets and Swiss Cheese Models (i.e. errors and systems) • 10 minutes discussion • Capture discussion on flip chart paper
Warfarin incident scenario 2 • Read through second page of the scenario • In your groups, discuss what could have prevented this incident • 10 minutes discussion • Capture discussion on flip chart paper
Yellow Book • Worked with BSH and patient group • Increased information and requirement to store records will require size to be A5 • Will incorporate credit card sized “alert card” with basic patient information • Space at back to store records of INR, dose, next clinic appointment (could be two part computerised form or hand written)
Competency development • NPSA developed the following sets of competencies using a Skills for Health framework: • Initiating anticoagulant therapy • Maintaining oral anticoagulant therapy • Managing anticoagulants in patients requiring dental surgery • Dispensing anticoagulants • Preparing and administering heparin therapy • Reviewing the safety and effectiveness of an anticoagulant service
Safety Indicators • Developed by the British Committee for Standards in Haematology (BCSH) and the NPSA • Compliment the guideline form BCSH on oral anticoagulation updated in 2006. • To be used as audit standards • A template (word document) for audit of Safety Standards can be downloaded from the BCSH website and modified for local use
Safety Indicators For Inpatients % patients following loading protocol % patients developing INR > 5 % patients in therapeutic range at discharge % patients suffering a major bleed in first month of therapy and percentage suffering major bleed with INR above therapeutic range % of new referrals to anticoagulant service with incomplete information % of patients that were not issued with patient held information and written dosage instructions at start of therapy % patients that were discharged from hospital without an appointment for next INR measurement or for consultation
Safety Indicators – Ambulatory Care Proportion of patient-time in range Percentage of INRs > 5.0 Percentage of INRs > 8.0 Percentage of INRs > 1.0 INR unit below target Percentage of patients suffering adverse outcomes Percentage of patients lost to follow up Percentage of patients with unknown diagnosis, target INR or stop date Percentage of patients with inappropriate target INR for diagnosis, high and low Percentage of patients without written patient educational information Completion of risk assessment of standard operating procedures
E-learning modules • Two e-learning modules commissioned • Initiating anticoagulant therapy • Maintaining patients on anticoagulant therapy • Aimed primarily at junior doctors • Will be available on the BMJ learning website
Safer Practice RecommendationsFor Anticoagulants Repeat prescriptions – check blood test results – on prescribing and dispensing Safer practice when co-prescribing an interacting medicine
Safer Practice RecommendationsFor Anticoagulants Safe management of patients requiring dental treatment Standardise the range/strengths of anticoagulants used Safe procedures for anticoagulants in care homes
Support materials • To aid implementation • Risk assessment tool, patient held information, posters, guidelines, protocols, work competences, e-learning modules, • To aid evaluation • Patient safety indicators, audit protocols and audit collection forms.
Juliet Brown wants to know what went wrong with her mother’s care… How would you communicate empathetically to the patient’s relatives?
Being open:Communicating with patients and/or carers about patient safety incidents Illustrative Workshop
Purpose of the Session • To provide an overview of the NPSA’s Being open policy and training • For participants to learn key communication skills that underpin effective communication with patients and/or carers following a patient safety incident.
NPSA’S Being open work • Being open policy • Safer Practice Notice • E-learning toolkit • One day training workshops
The Ten Principles 1. Acknowledgement 2. Truthfulness, timeliness and clarity of communication 3. Apology 4. Recognising patient and/or carer expectations 5. Professional support 6. Risk management and systems improvement 7. Multidisciplinary responsibility 8. Clinical governance 9. Confidentiality 10. Continuity of care
Actions for healthcare organisations • Develop and implement a local Being open policy by June 2006. • Identify local Being open leads and clinicians to attend Being open training workshops. • Raise awareness of the Being open e-learning locally and ensure staff have access to it.