Download
1 / 22
230 likes | 430 Views
Pleural Effusion and +PPD. Sandy Valmadrid, MD 13 December 2006. Case. EH, 56 yo nonsmoker Shortness of breath, fever, night sweats Dc’d 3 days ago, St. Mary’s Hospital 102 fever, sob, cough WBC 19.3, neutrophilic predominance Cxray: RLL pneumonia Sputum: Streptococcus pneumoniae

E N D
Pleural Effusion and +PPD Sandy Valmadrid, MD 13 December 2006
Case • EH, 56 yo nonsmoker • Shortness of breath, fever, night sweats • Dc’d 3 days ago, St. Mary’s Hospital • 102 fever, sob, cough • WBC 19.3, neutrophilic predominance • Cxray: RLL pneumonia • Sputum: Streptococcus pneumoniae • Moxifloxacin, O2, LOS 7 days
…case continued • Comorbidities: • Chronic Venous Insufficiency, bipedal edema • Mild MR, TR, EF 65% • DVT, chronic anticoagulation • Anemia Hct 28%, recent dental bleeding • DM 2, diet controlled • Hypertension • Abdominal Hernia • Obese (BMI 37), Chronic OA pains
…case continued • Medications • Furosemide 40 mg, KCl 20 meq QAM • Warfarin 5 mg QPM • ? Atenolol 50 mg QAM • Amlodipine 10 mg QAM • Clonidine 200 mcg QAM • PRN Acetaminophen/Codeine QID • PRN Zolpidem, OTC’s
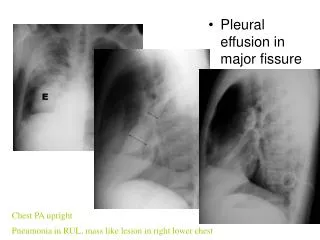
…case continued • sob, sweats • 148/70, 104 bpm, 26 bpm, 99.2 F • O2 sats RA 87%, with 2Li 96% • Pale, coughing, short sentences • decreased bibasilar breath sounds, depth rhonchi clears with cough • CXray: small bibasilar effusions, R>L • Moxifloxacin, O2, incentive spiro, watch
…case continued • +2 weeks • Feels “worse,” some sob, sweats, nonproductive cough • O2 sats RA 95%, 97.8 F • WBC 9.3 • CXray: mod sized R pleural effusion, small L • Pneumonia with parapneumonic effusion or something else
Pleurocentesis WBC 2,175 Neut 0% Lymph 80% Mphag 9% Eos 3% 0thers 0% RBC 23,150 Protein 5.2 (s8.0) LDH 198 (s240) GS and Cultures Negative AFB not done Cytology Negative ?? Infection, TB, mesothelioma, malignancy, PE …case continued
…case continued • +TST skin test 20 mm • CT Thorax • R pleural effusion, small • RUL nodular (up to 14 mm) airspace disease w/ surrounding ground glass pattern • <1cm paratracheal and axillary lymphnodes • Minimal pericardial effusion
…case continued • ??Active TB • 3 sputum AFB samples Negative • Pulmonary Clinic: Bronchoscopy if negative
…case continued • While working on diagnostics, • Clinically improved • Less compliant • HIV test negative, Hep C positive • Review of history • ? Mother or relative with active TB, 70’s • ? Positive skin test or treatment in the past • Repeat CT - resolving nodules/effusion
…case continued • NO active TB • Resolving CT scan and respiratory symptoms, HIV negative • YES Latent TB Infection (LTBI)
Objectives • Update on LTBI • TB Epidemiology • Making the diagnosis • Treatment
TB Burden • Airborne Mycobacterium tuberculosis has infected humans since ancient times • WHO Worldwide Estimates: • ~ 1.9 billion infected • ~ 16 million active cases • ~ 6 million new cases every year • ~ 1.7 million deaths every year
…TB Burden continued • US estimates • ~ 26,000 cases/year - late 80’s, early 90’s a resurgence attributed to HIV and multidrug resistant TB • ~ 15,000 cases/year – 2001 • Treatment of LTBI in moderate to high risk patients reduces risk of developing active TB by up to ~70%
LTBI(Latent TB Infection) • After the primary TB infection • Up to 85% - Infection eradicated • Up to 5% - Progress to active TB; much higher % in HIV and other risk groups • Up to 5% - LTBI or those who temporarily control infection only to fail at a later time (“endogenous reactivation”)
LTBI diagnosis • Identify moderate to high risk groups • Test (TST, Quantiferon G) • R/O Active TB
Tuberculin Skin Test Issues administering, interpreting Difficult with BCG or other mycobacterium sp. Cheaper? $40-70 facility charge + $13.70 test ELISA or ELISPOT (Quantiferon, T Spot-TB) Easier No booster phenomenon Better Specificity, PPV Comparable? $15-18 venipunture $87-123 test …LTBI Diagnosis
…LTBI Diagnosis • R/O Active TB • Hx, PE • PA Chest Xray • (-) = LTBI - Treat LTBI • (+) OR (-) and HIV/chr respiratory ssx Obtain 3 Sputum samples (AFB, NAA, cultures): • Sputum (-), Low suspicion – Treat LTBI • Sputum (-), High suspicion - Treat Active TB until cultures out • Culture (+) – continue treat Active TB • Culture (-) , cxray improving – continue treat Active TB • Sputum (+) - Treat Active TB
Case revisited • EH qualifies as having LTBI • Two hurdles to successful treatment • Compliance • High risk for adverse reactions • Ask help from ID • Would Quantiferon help? • Suspect 4 mo. RIF or 6 mo INH with Directly Observed Therapy and close LFT monitoring
References • http://www.thoracic.org • http://findtbresources.org • CDC. Guidelines for using the QuantiFERON-TB Gold Test for detecting Mycobacterium tuberculosis infection, United States. MMWR 2005;54(No.RR-15):49-55 • American Thoracic Society, CDC. Targeted tuberculin testing and treatment of latent tuberculous infection. Am J Respir Crit Care Med 2000:161:S221-47.