Download
1 / 80
800 likes | 823 Views
Grazie per aver scelto di utilizzare a scopo didattico questo materiale delle Guidelines 2011 libra. Le ricordiamo che questo materiale è di proprietà dell’autore e fornito come supporto didattico per uso personale. ORIGINS of ASTHMA. G E N E T I C. Lung Development

E N D
Grazie per aver scelto di utilizzare a scopo didattico questo materiale delle Guidelines 2011 libra.Le ricordiamo che questo materiale è di proprietà dell’autore e fornito come supporto didattico per uso personale.
ORIGINS of ASTHMA G E N E T I C • Lung Development • Immunologic Maturation • Allergens • Exposure to Tobacco Smoke • Other adjuvant factors • Diet • Psychological factors • Conclusions E N V I R O N M E N T Attilio Boner University of Verona, Italy attilio.boner@univr.it
Lung development Bronchial development complete by the 16° week True alveoli begin to develop at 28 weeks and increase in number, size and complexity during the first 3-4 years of life. Dysanaptic growth and Traking of lung function
TUCSON CHILDREN’S RESPIRATORY STUDY: 1980 TO PRESENT Taussig JACI 2003; 111:661 HYPOTHETICAL PEAK PREVALENCE BY AGE FOR THE 3 DIFFERENT WHEEZING PHENOTYPES. ALB
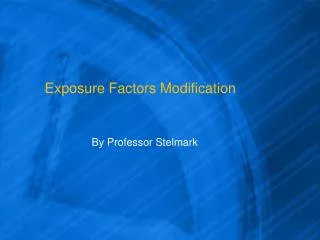
LUNG FUNCTION ACCORDING TO WHEEZING HISTORY AT 6 YEARS AT: Early infancy 6 years of age V max of FRC (ml/s) V max of FRC (ml/s) 160- 140- 120- 100- 80- 60- 40- 20- 0 - 1400- 1300- 1200- 1100- 1000- 900- 800 - - - - - - - - - - - - * * - - - *p<0.05 *p<0.05 never early transient wheezers late persistent never persistent early transient wheezers late Martinez NEJM 1995;332:133
TUCSON CHILDREN’S RESPIRATORY STUDY: 1980 TO PRESENT Taussig JACI 2003; 111:661 ? HYPOTHETICAL PEAK PREVALENCE BY AGE FOR THE 3 DIFFERENT WHEEZING PHENOTYPES. ALB
ALB WHEEZY BRONCHITIS IN CHILDHOOD. A DISTINCT CLINICAL ENTITY WITH LIFELONG SIGNIFICANCE? Edwards Chest 2003;124:18 Mean decline FEV1 (L) between 1989 and 2001 WHEEZY BRONCHITIS • A cohort of children originally studied in 1964 was revaluated in 2002 (age 45-50) n=283 CONTROL ASTHMA 0 -10- -20- -30- -40- -50- -60- -70- -80- -0.75 (L) -0.75 (L) -0.59 (L) p<0.01
Early life origins of chronic obstructive pulmonary disease Svanes Thorax 2010;65:14–20 • European Community Respiratory Health Survey participants aged 20–45 years randomly selected from general populations. • Spirometry in 1991–3 (n=13,359) and 9 years later (n=7,738). defined as ‘‘childhood disadvantage factors’’. • Maternal asthma, • Paternal asthma, • Childhood asthma, • Maternal smoking and • Childhood respiratory infections
Early life origins of chronic obstructive pulmonary diseaseSvanes Thorax 2010;65:14–20 OR for FEV1/FVC ≤ 70% 8 – 7 – 6 – 5 – 4 – 3 – 2 – 1 – 0 7.2 6.3 1.7 1.6 ≥3 1 ≥3 1 n°FACTORS IN MEN n°FACTORS IN WOMEN
alb HYPOTHETICAL YEARLY PEAK PREVALENCE OF WHEEZING ACCORDING TO PHENOTYPE IN CHILDHOOD Martinez F., Pediatrics 2002; 109: 362 Transient early wheezers Non-atopic wheezers IgE-associated wheeze/asthma Wheezing prevalence 0 6 11 3 Age (years)
REDUCED LUNG FUNCTION BOTH BEFORE BRONCHIOLITIS AND AT 11 YRS Turner Arch Dis Child 2002; 87: 417 . %VmaxFRC 3 2 1 0 p=0.02 • 253 cohort members • VmaxFRC at 1 month of age • Individuals with bronchiolitis were prospectively identified • At 11 years of age lung function was repeated . z score -1 -2 -3 Confirmed bronchiolitis (n = 16) Control (n = 162) Box and whisker plot for z scores for % V’maxFRCat 1 month
ALB TUCSON CHILDREN’S RESPIRATORY STUDY: 1980 TO PRESENT Taussig JACI 2003; 111:661 HYPOTHETICAL PEAK PREVALENCE BY AGE FOR THE 3 DIFFERENT WHEEZING PHENOTYPES.
Lung function according to wheezing history at 6 years at: Martinez NEJM 1995; 332: 133 Early infancy 6 years of age V max of FRC (ml/s) V max of FRC (ml/s) 160- 140- 120- 100- 80- 60- 40- 20- 0 - 1400- 1300- 1200- 1100- 1000- 900- 800 - - - - - - - - - - - - - - - never early late persistent never early persistent late wheezers wheezers
Z score VmaxFRC THE RELATIONSHIP BETWEEN INFANT AIRWAY FUNCTION, CHILDHOOD AIRWAY RESPONSIVENESS, AND ASTHMA Turner-Le Souef AJRCCM 2004; 169: 921 2 1 0 p=0.02 • VmaxFRC was assessed at 1 month of age • The presence of wheeze up to 11 years of age was prospectively identified • At 11 years of age, airway responsiveness (AR) to inhaled histamine and atopy were assessed -1 -2 PW n=17 NW n=67 W 4-6 n=41 W 11 n=6 W 0-3 n=26 Box and whisker plot showing median and quartiles values for Z scores of VmaxFRC at 1 month in groups defined by wheeze at different ages.
REDUCED LUNG FUNCTION AT BIRTH AND THE RISK OF ASTHMA AT 10 YEARS OF AGE Haland , Carlsen N Engl J Med 2006; 355: 1682 % children with a history of asthma at age 10 year % children with current asthma at age 10 year 30 – 20 – 10 – 0 30 – 20 – 10 – 0 p=0.01 24.3% p=0.005 16.2% 14.6% 7.5% Above the median At-below the median Above the median At-below the median tPTEF/tE at age 3 days tPTEF/tE at age 3 days
ORIGINS of ASTHMA • Lung Development • Reduced lung development is a • premorbid predisposing factor for: • Transient wheezing, • Bronchiolitis, • Persistent atopic wheezing, Attilio Boner University of Verona, Italy
ORIGINS of ASTHMA G E N E T I C • Lung Development • Immunologic Maturation • Allergens • Exposure to Tobacco Smoke • Other adjuvant factors • Diet • Psychological factors • Conclusions E N V I R O N M E N T Attilio Boner University of Verona, Italy attilio.boner@univr.it
alb MATERNO-PLACENTO-FETAL INTERACTIONS Warner Arch Dis Child 2004;89:97 One of the explanations for maintenance of a successful pregnancy is that both Th-2 (IL-4 and IL-13) and T regulatory (IL-10 and TGF-β) cytokines are generated by the conceptus to down-regulate maternal Th-1 immune responses to feto-paternal antigens which might otherwise lead to fetal rejection. 22°wk 14°wk
SENSITIZATION DOES NOT DEVELOP IN UTERO Bonnelykke JACI 2008;121:646 • Inhalant and food allergen-specific IgE in cord blood and in infant blood at 6 months of age and in parental blood; • Cord blood IgA was measured to detect maternal blood contamination of cord blood. % of cord blood with (+) sIgE 15 – 10 – 5 – 0 14%
SENSITIZATION DOES NOT DEVELOP IN UTERO Bonnelykke JACI 2008;121:646 • Inhalant and food allergen-specific IgE in cord blood and in infant blood at 6 months of age and in parental blood; • Cord blood IgA was measured to detect maternal blood contamination of cord blood. % of cord blood with (+) sIgE However, corresponding specific IgE was not found in infant blood at 6 months of age. 15 – 10 – 5 – 0 14%
PRENATAL VERSUS POSTNATAL SENSITIZATION TO ENVIRONMENTAL ALLERGENS IN A HIGH-RISK BIRTH COHORT Rowe JACI 2007;119:1164 • Prospectively studied HDM (house dust mite) specific sIgE and IgG4 and T-cell immunity in a cohort of 200 high-risk infants 0.35 Age (months) Tracking antibody titers in individuals who are HDM SPT-positive at age 24 months
SKIN BARRIER FUNCTION AND ALLERGIC RISK Hudson Nature Genetics 2006; 38: 399 Skin barrier function and allergic risk. An intact epithelial barrier (a) prevents allergens from reaching antigen presenting cells (APCs) in subepithelial tissues. Damage to this barrier (b) allow allergens to penetrate into the subepidermal layer and interact with APCs, leading to allergic sensitization and, secondarily, to allergic manifestations in the host.
FILLAGRIN LOSS-OF-FUNCTION MUTATIONS PREDISPOSE TO PHENOTYPES INVOLVED IN THE ATOPIC MARCH Marenholz JACI 2006; 118: 866 OR ratio for concomitant eczema and asthma OR ratio for concomitant eczema and allergic rhinitis 7 – 6 – 5 – 4 – 3 – 2 – 1 – 0 OR for non atopic eczema OR for atopic eczema 6.21 4.79 3.94 3.84 p=0.00001 p=0.0006 p=0.00001 p=0.00065 IN CHILDREN WITH FILAGGRIN LOSS-OF-FUNCTION MUTATION
A pilot study of emollient therapy for the primary prevention of atopic dermatitis. Simpson EL, J Am Acad Dermatol. 2010;63:587-93. 50 – 40 – 30 – 20 – 10 – 0 • 22 neonates at high risk for developing AD • emollient therapy from birth. • followed up mean time of 547 days % children who developed AD 15%
A pilot study of emollient therapy for the primary prevention of atopic dermatitis. Simpson EL, J Am Acad Dermatol. 2010;63:587-93. Chance of developing AD in similar high-risk infants 50 – 40 – 30 – 20 – 10 – 0 50% • 22 neonates at high risk for developing AD • emollient therapy from birth. • followed up mean time of 547 days 30% % children who developed AD Hoare C, Health Technol Assess 2000;4:1-191. 15%
A pilot study of emollient therapy for the primary prevention of atopic dermatitis. Simpson EL, J Am Acad Dermatol. 2010;63:587-93. 50 – 40 – 30 – 20 – 10 – 0 • 22 neonates at high risk for developing AD • emollient therapy from birth. • followed up mean time of 547 days No side effect Effects on atopic asthma development? % children who developed AD 15%
ORIGINS of ASTHMA • Lung Development • Immunologic Maturation The fetal life and the newborn period are prone to atopy. Sensitization starts early but postnataly. Defective skin barrier fuction predispose to allergy development. Attilio Boner University of Verona, Italy
ORIGINS of ASTHMA G E N E T I C • Lung Development • Immunologic Maturation • Allergens • Exposure to Tobacco Smoke • Other adjuvant factors • Diet • Psychological factors • Conclusions E N V I R O N M E N T Attilio Boner University of Verona, Italy attilio.boner@univr.it
Early life risk factors for adult asthma: a birth cohort study of subjects at risk Rhodes H.L JACI 2001; 108: 721 ODD ratio for adult asthma 11- 10- 9- 8- 7- 6- 5- 4- 3- 2- 1- 0 • Cohort study • 100 babies of atopic parents • Followed - at 5 yrs, - at 11 yrs, - at 22 yrs 10.7 (+) SPT for egg or milk in the first year
Early life risk factors for adult asthma: a birth cohort study of subjects at risk Rhodes H.L JACI 2001; 108: 721 ODD ratio for adult asthma 11- 10- 9- 8- 7- 6- 5- 4- 3- 2- 1- 0 • Cohort study • 100 babies of atopic parents • Followed - at 5 yrs, - at 11 yrs, - at 22 yrs 10.7 (+) SPT for egg or milk in the first year
10 – 9 – 8 – 7 – 6 – 5 – 4 – 3 – 2 – 1 – 0 to perennial allergen ALB PERENNIAL ALLERGEN SENSITISATION EARLY IN LIFE AND CHRONIC ASTHMA IN CHILDREN: A BIRTH COHORT STUDY Illi Lancet 2006; 368: 763 OR for BHR at school age 8.3 • 1314 children from birth to 13 years of age (MAS study) • Allergen exposure at age 6 months, 18 months, and at 3, 4, and 5 yrs • Lung function at 7, 10, and 13 yrs 3.29 Early Current sensitization sensitisation (age <3)
THE CANADIAN CHILDHOOD ASTHMA PRIMARY PREVENTION STUDY: OUTCOMES AT 7 YEARS OF AGE Chan-Yeung JACI 2005; 116: 49 % ch. with pediatric diagnosis of asthma 30 – 20 – 10 – 0 • 545 high-risk infants with immediate FH of asthma and allergies • Intervention (avoidance of house dust) or control groups • Outcomes at 7 years 23% p=0.006 14.9% OR = 0.44 Intervention Controls
p=0.005 PREVENTION OF ALLERGIC DISEASE DURING CHILDHOOD BY ALLERGEN AVOIDANCE: THE ISLE OF WIGHT PREVENTION STUDY Arshad JACI 2007;119:307 • Infants at higher risk because of family predisposition. • Randomized to prophylactic (n=58) and control (n=62) groups. • Prophylactic group: breast-fed or extensively hydrolyzed formula, acaricide and mattress covers. • Development of allergic disease at age 1,2,4 and 8 years. OR in the prophylactic group at age 8 years 1 – 0,5 – 0 0.24 0.23 0.14 0.13 p=0.005 p=0.0003 p<0.005 asthma Atopic dermatitis atopy Allergic rhinitis
ALB EARLY LIFE ENVIROMENTAL CONTROL: EFFECT ON SYMPTOMS, SENSITIZATION AND LUNG FUNCTION AT AGE 3 YEARSWoodcock AJRCCM 2004;170:433 1.0 – 0.8 – 0.6 – 0.4 – 0.2 – 0.0 Ln VmaxFRC GM & 95% CI at age 4 weeks * • Manchester cohort • 128 active group • 111 control group • Allergen level, symptoms, sensitization and lung function at 3 years of age * p=0.49
ALB EARLY LIFE ENVIROMENTAL CONTROL: EFFECT ON SYMPTOMS, SENSITIZATION AND LUNG FUNCTION AT AGE 3 YEARSWoodcock AJRCCM 2004;170:433 Ln sRaw GM & 95% CI at age 3 years * • Manchester cohort • 128 active group • 111 control group • Allergen level, symptoms, sensitization and lung function at 3 years of age 0.4 – 0.3 – 0.2 – 0.1 – 0.0 – -.1 * p=0.003
EARLY LIFE ENVIROMENTAL CONTROL: EFFECT ON SYMPTOMS, SENSITIZATION AND LUNG FUNCTION AT AGE 3 YEARSWoodcock AJRCCM 2004;170:433 Ln sRaw GM & 95% CI at age 3 years * • Manchester cohort • 128 active group • 111 control group • Allergen level, symptoms, sensitization and lung function at 3 years of age 0.4 – 0.3 – 0.2 – 0.1 – 0.0 – -.1 This may be an important factor in relation to the traking effect of lung function * p=0.003
A LONGITUDINAL, POPULATION-BASED, COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD.Sears NEJM 2003;349:1414 100 – 90 – 80 – 70 – 60 – 50 – 40 – 30 – 20 – 10 – 0 • 1139 newborn (April 1972-March 1973); • Assessed at 3 yrs, every 2 yrs up to 15 yrs than at 18, 21, and 26 yrs of age; • Questionnaire; • Lung function; • SPT, sIgE; • Methacholine ch. % SUBJECTS AT 26 YEARS 72.6 51.4 26.9 WHEEZING ONCE >ONCE CURRENTLY
A LONGITUDINAL, POPULATION-BASED, COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD.Sears NEJM 2003;349:1414 % SUBJECTS AT 26 YEARS 30 – 20 – 10 – 0 • 1139 newborn (April 1972-March 1973); • Assessed at 3 yrs, every 2 yrs up to 15 yrs than at 18, 21, and 26 yrs of age; • Questionnaire; • Lung function; • SPT, sIgE; • Methacholine ch. 12.4% HAD REMISSION FOLLOWED BY RELAPSE BY AGE 26 26.9 14.5 WHEEZING CURRENTLY PERSISTENT
A LONGITUDINAL, POPULATION-BASED, COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD.Sears NEJM 2003;349:1414 OR FOR WHEEZING AT AGE 26 YEARS 5 - 4 - 3 – 2 – 1 – 0 p<0.001 for trend 4.17 FOR RELAPSE 3.38 FOR PERSISTANCE (+) SPT FOR MITES AT AGE 13 YEARS
ORIGINS of ASTHMA • Lung Development • Immunologic Maturation • Allergens • Early sensitization to allergens is a risk factor for more severe asthma and reduced lung function, • Sensitization may occur through the skin, • Sesitization can occur also later in life and is always a risk factor for asthma Attilio Boner University of Verona, Italy
ORIGINS of ASTHMA G E N E T I C • Lung Development • Immunologic Maturation • Allergens • Exposure to Tobacco Smoke • Other adjuvant factors • Diet • Psychological factors • Conclusions E N V I R O N M E N T Attilio Boner University of Verona, Italy attilio.boner@univr.it
SMOKING MOTHER THE EFFECT OF MATERNAL SMOKING DURING PREGNANCY ON EARLY INFANT LUNG FUNCTION Hanrahan Am. Rev. Respir. Dis. 1992; 145: 1129 Flow at functional residual capacity (ml/s) 200 – 150 – 100 – 50 – 0 • 80 healthy infants tested shortly after birth (mean, 4.2+/-1.9 wk) • Urine cotinine • Expiratory flow-volume curves p= 0.0007 150.4 74.3 YES NO
MATERNAL AND GRANDMATERNAL SMOKING PATTERNS ARE ASSOCIATED WITH EARLY CHILDHOOD ASTHMA Li YF Chest 2005; 127: 1232 OR for asthma in the first 5 years of life 3 – 2 – 1 – 0 2.6 • 338 children with asthma diagnosed in the first 5 years of life • 570 control subjects 1.8 1.3 Grandmaternal only smoking during the mother’s fetal period Grandmaternal and maternal smoking Smoking mother only
THE ADULT INCIDENCE OF ASTHMA AND RESPIRATORY SYMPTOMS BY PASSIVE SMOKING IN UTERO OR IN CHILDHOOD Skorge AJRCCM 2005; 172: 61 OR ratio for adult onset asthma 3 – 2 – 1 – 0 • Between 1985 and 1996/1997 an 11-year community cohort study on the incidence of asthma • 3.786 subjects 3 Smoking mother
THE ADULT INCIDENCE OF ASTHMA AND RESPIRATORY SYMPTOMS BY PASSIVE SMOKING IN UTERO OR IN CHILDHOOD Skorge AJRCCM 2005; 172: 61 The adjusted attributable fractions of the adult incidence of asthma were 17.3% caused by maternal smoking and 9.3% caused by smoking by other household members. OR ratio for adult onset asthma 3 – 2 – 1 – 0 • Between 1985 and 1996/1997 an 11-year community cohort study on the incidence of asthma • 3.786 subjects 3 Smoking mother
REGULAR SMOKING AND ASTHMA INCIDENCE IN ADOLESCENTS Gilliland AJRCCM 2006; 174: 1094 RR FOR NEW ONSET OF ASTHMA • 2,609children with no lifetime history of asthma or wheezing • Followed annually in schools • Regular smoking was defined as smoking 300 cigarettes in the year • New cases of physician-diagnosed asthma 4 – 3 – 2 – 1 – 0 3.9 In children smoking >300 cigarettes/year
REGULAR SMOKING AND ASTHMA INCIDENCE IN ADOLESCENTS Gilliland AJRCCM 2006; 174: 1094 RR FOR NEW ONSET OF ASTHMA 10- 8 – 6 – 4 – 2 – 0 • 2,609children with no lifetime history of asthma or wheezing • Followed annually in schools • Regular smoking was defined as smoking 300 cigarettes in the year • New cases of physician-diagnosed asthma 8.8 In children smoking >300 cigarettes/year and exposed to maternal smoking during gestation
ORIGINS of ASTHMA • Lung Development • Immunologic Maturation • Allergens • Exposure to Tobacco Smoke Smoking should always be avoided by anyone. Attilio Boner University of Verona, Italy
ORIGINS of ASTHMA G E N E T I C • Lung Development • Immunologic Maturation • Allergens • Exposure to Tobacco Smoke • Other adjuvant factors • Diet • Psychological factors • Conclusions E N V I R O N M E N T Attilio Boner University of Verona, Italy attilio.boner@univr.it