Download
1 / 14
270 likes | 1.71k Views
Management of Enterocutaneous Fistulae. Mary Arnold Long , MSN, RN, CRRN, CWOCN-AP, ACNS-BC Clinical Nurse Specialist Wound, Ostomy , Continence Roper Hospital Charleston, SC. Colorectal Symposium March 16, 2013. What is an Enterocutaneous Fistulae?.

E N D
Management of Enterocutaneous Fistulae Mary Arnold Long, MSN, RN, CRRN, CWOCN-AP, ACNS-BC Clinical Nurse Specialist Wound, Ostomy, Continence Roper Hospital Charleston, SC Colorectal Symposium March 16, 2013
What is an Enterocutaneous Fistulae? • A connection between the small intestine andthe skin • May also be entero – atomospheric (between small intestine and air) • May be related to diseases (e.g. Crohn’s, diverticulitis), trauma or surgery complications • Results in spillage of fecal contents from small intestine onto skin
What are Types of Enterocutaneous Fistulae? • Acute = less than 30 days old • Chronic = more than 30 days old • Low volume= <200cc/24 hours • Moderate volume= 200-500cc/24 hours • High volume = >500cc/24 hours
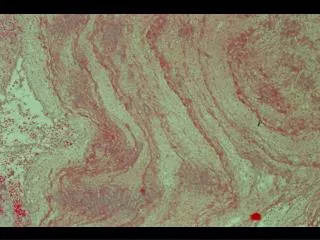
Acute enterocutaneous fistula after tube cecostomy Chronic stomatized gastro-atmospheric fistula
How do you Manage an Enterocutaneous Fistulae? Suction Complex fistula Increase wear time Combination • Dressings • If lower volume output • Pouching • If higher volume output • To quantify output
What are the Goals for Enterocutaneous Fistula Management? • Protect Skin • Contain Drainage • Manage Nutrition • Manage Hydration • Manage Odor • Psychosocial Needs
Pouching a Fistula • Cleanse & dry wound and periwound skin. • Protect periwound skin with No Sting skin sealant. • Protect periwound skin with barrier wafer or hydrocolloid (Duoderm, etc.) & ostomy paste because you cut the pouch opening LARGER than the wound/fistula to prevent undermining. • If the fistula is active, it helps to have another person suction the effluent while you’re working to keep the skin free of drainage.
Remove & discard old dressing. Cleanse wound & skin. Protect periwound skin with NoSting skin sealant. Place contact layer (Adaptic, Mepitel, etc.) to wound base. Fill wound with fluffed gauze. Place tube (with large holes cut into it) over gauze. This tube can be a large bore catheter. Using Suction on a Fistula
7. Secure dressing with transparent film (Tegaderm, OpSite). 8. Add ostomy paste beneath film to promote seal prn. 9. Use tape to border edges prn. 10. Connect drain tube to cannister tubing. Use 5-in-1 adapter if needed. 11. Tape connections prn. 12. Verify suction tubing connected to cannister. 13. Turn on low continuous suction. 14. Monitor & modify settings prn. 15. Irrigate prn. Using Suction on a Fistula
1. Cut extra holes in thetube you will use as the drain. This can be a large bore catheter. 2. Insert the drain into the pouch and secure it. DO NOT have the drainresting directly on the wound or fistula. 3. Connect the drain to suction. 4. Follow directions 10-15 for “Using Suction on a Fistula.” Adding Suction to a Pouch
The Roper WOC RNs Resources for Our Patients AND for You!!