Download
1 / 57
671 likes | 1.08k Views
12-Lead EKG MEPN Level IV. OBJECTIVES. Discuss the changes in T wave and ST segment morphology with an MI List the criteria for identification of right or left bundle branch blocks. List the anatomically congruent leads associated with an inferior, lateral and anterior wall MI

E N D
12-Lead EKG MEPN Level IV
OBJECTIVES • Discuss the changes in T wave and ST segment morphology with an MI • List the criteria for identification of right or left bundle branch blocks. • List the anatomically congruent leads associated with an inferior, lateral and anterior wall MI • Describe morphology of Q wave presence
ECG Leads • 6 limb leads (frontal plane) • 3 bipolar leads • 3 unipolar leads • 6 precordial leads (horizontal plane) • V1 – V6
Einthoven’s Triangle Limb Leads BIPOLAR • Lead I • RA (-) to LA (+) • Lead II • RA (-) to LL (+) • Lead III • LA (-) to LL (+)
AUGMENTED (UNIPOLAR) LEADS Augmented leads combine 2 leads together (the null point) from the center point of the triangle with one positive pole. aVR (Augmented Voltage Right Arm positive) is a combination of bipolar Leads I and II aVL (Augmented Voltage Left Arm Positive) is a combination of I and III aVF (Augmented Voltage Left Foot positive) is a combination of Bipolar Leads II and III
I & AVL II, III & AVF WHAT ARE THE LEADS LOOKING AT? LIMB and AUGMENTED LEADS
Precordial Lead Placement • V1 – 4th intercostal space right of sternum • V2 - 4th intercostal space left of sternum • V4 – 5th intercostal space midclavicular line • V3 – midway between V2 and V4 • V6 – 5th intercostal space midaxillary line • V5 – same level as V4 at anterior axillary line between V4 and V6
RIGHT SIDED EKG Same lead position as left side – looks directly at the Right ventricle
Posterior View Posterior leads: V7 – lateral to V6 at posterior axillary line V8 – level of V7 at the mid-scapular line V9 – level of V8 at the paravertebral line (left posterior thorax midway from spine to V8)
V3 & V4 V1 & V2 V5 & V6 PRECORDIAL LEADS
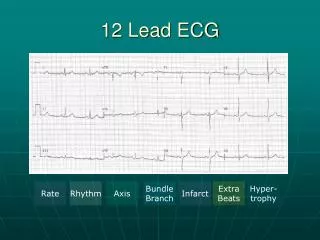
calibration marker LIMB LEADS AUGUMENTED LEADS PRECORDIAL LEADS Bottom line is continuous strip
Myocardial ischemia • Various definitions are used. The term commonly refers to diffuse ST segment depression, usually with associated T wave inversion • Myocardial injury • Injury always points outward from the surface that is injured with ST segment elevation
ST Segments ST segment should be electrically neutral
Visual aid in determining: • Ischemia or injury to myocardium • Normal should be at baseline • Depressed ST segment - >2 mm below baseline
ST Segment Elevation • ST segment elevation is attributed to impending infarction • but can also be due to pericarditis or vasospastic (variant) angina. • The height of the ST segment is measured at a point 2 boxes after the end of the QRS complex • significant if it exceeds 1 mm in a limb lead or 2 mm in a precordial lead.
T Waves • T waves are normally positive in leads with a positive QRS • T waves are normally asymmetrical • T waves are normally not more than 5 mm high in limb leads or 10 mm high in precordial leads or 2/3 the height of the R wave
T wave Ischemia Ischemia Hyperkalemia Ischemia
Hyperkalemia EKG 3
ST-T Wave • Combination of infarction and often hyperkalemia • Called Tombstone ‘T’ because of the shape. • Usually a sign of impending cardiac death.
Localization of ECG Pathology • Inferior: Abnormalities that appear in leads II, III, and aVF (called the inferior leads) indicate pathology on the inferior or diaphragmatic surface of the heart. • Lateral:Leads I, aVF, and V5-V6 are called lateral leads. Abnormality in these leads indicates pathology on the lateral, upper surface of the heart. • Anterior: Anterior pathology is seen in leads V1-V4, and often in lead I.
T Wave Elevation T STSegment Elevation ST ST Q T Pathological Q Wave Q Q T T WaveInversion
EKG Changes from Infarction • First Detectable Change in EKG • Tall T-waves • increase in height • more symmetric • may occur in the first few minutes Hyper-acute Phase
Acute Phase • ST Segment Elevation • Primary indication of injury • Occurs in first hour to hours • ST Segment Elevation in Leads • 1mm or greater in limb leads • 2 mm or greater in chest leads • Hallmark indication of AMI
View of Inferior Heart Wall • Leads II, III, aVF • Looks at inferior heart wall
Inferior EKG 5
Inferior EKG 6
View of Lateral Heart Wall • Leads I and aVL • Looks at lateral heart wall • Looks from the left arm toward heart *Sometimes referred to as High Lateral or High Apical view*
View of Lateral Heart Wall • Leads V5 & V6 • Looks at lateral heart wall • Looks from the left lateral chest toward heart *Sometimes referred to as Low Lateral or Low Apical view*
Lateral Wall View of Entire Lateral Heart Wall Leads I, aVL, V5, V6 - Looks at the lateral wall of the heart from two different perspectives
Lateral EKG 7
Lateral EKG 8
View of AnteriorHeart Wall • Leads V3, V4 • Looks at anterior heart wall • Looks from the left anterior chest
Anterior EKG 9
Anterior EKG 10
View of Septal Heart Wall • Leads V1, V2 • Looks at septal heart wall • Looks along sternal borders
Putting it ALL together ANTERIOR LATERAL S E P T A L LATERAL LATERAL INFERIOR
Q Waves • Definition • Septal depolarization • Normally present in I, aVL, V6
Two types of Q waves • Non-pathologic • Narrow, shallow Q waves • Not visible in all leads • Pathologic • > 0.04 in duration; at least 1/4 to 1/3 height of R wave • Represent an infarcted area of myocardium