Download
1 / 12
120 likes | 239 Views
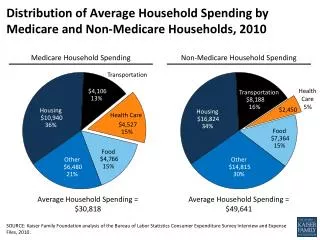
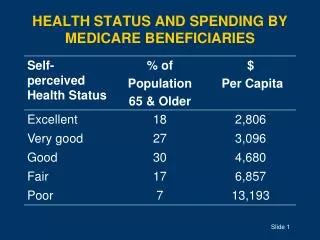
HEALTH STATUS AND SPENDING BY MEDICARE BENEFICIARIES. THE 65+ AGE GROUP INCLUDES MANY HEALTHY PEOPLE Percentage Reporting Good to Excellent Health. Source: Medicare Current Beneficiary Survey , 1997, Table 2.3. THE RISK OF DISABILITY INCREASES WITH AGE.

E N D
THE 65+ AGE GROUP INCLUDES MANY HEALTHY PEOPLEPercentage Reporting Good to Excellent Health Source:Medicare Current Beneficiary Survey, 1997, Table 2.3
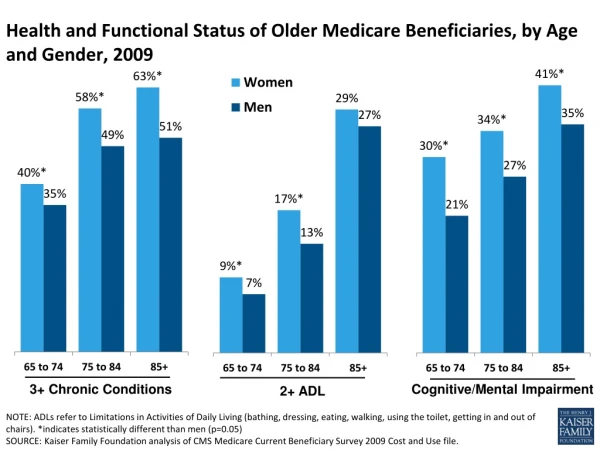
THE RISK OF DISABILITY INCREASES WITH AGE Note: ADLs = activities of daily living; IADLS = instrumental ADLs. Source: Medicare Current Beneficiary Survey, 1997, Table 2.1.
TRENDS IN NURSING HOME USE • Supply of beds per 1000 people is shrinking: 1987: 141 1996: 117 • % of Americans aged 65+ living in nursing homes has remained constant, at 5% • Lifetime chance of ever living in a nursing home is rising • Nursing-home population is older and more dependent Source: Cobbs EL, Duthie EH,Murphy JB, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine. 5th ed. Malden MA: Blackwell Publishing for the AGS; 2002, p.13.
THE RISK OF MORBIDITY & MORTALITY RISES WITH: • Failure to report symptoms • Atypical presentation • Maladaptation to environmental change • Adverse drug reactions
ATYPICAL PRESENTATIONS IN OLDER PATIENTS • Functional decline e.g., falls, confusion, weight loss • Misleading symptoms e.g., pneumonia with low fever & low WBC count • Signs of one disease obscured by another e.g., COPD worsened by CHF • No presentation at all e.g., silent infarct, painless acute abdomen
IATROGENIC ILLNESS IS COMMON AMONG OLDER PATIENTS • Nearly 1 in 3 acutely hospitalized older patients • Adverse drug reactions are the most common iatrogenic illness • Other complications of hospitalization: • deconditioning • delirium • falls • infection • pressure ulcers • Results are functional losses and increased costs
TOP 5 CAUSES OF DEATH AMONG OLDER AMERICANS IN 1999 Source: National Vital Statistics Report, vol. 49, no. 11 (October 12, 2001), p. 15, Table 1.
THE RISK OF COGNITIVE DISORDER IS HIGHER FOR OLDER PATIENTS • Prevalence of dementia increases with age • Chronic illness is often accompanied by cognitive and affective disorders • Up to 20% to 30% of hospitalized older patients develop delirium • Dementia, delirium, and depression have overlapping symptoms, increasing the difficulty of diagnosis
SOCIAL SUPPORTS CAN BE THE KEY TO PRESERVING FUNCTION • Economic status • Marital status & living arrangements • Caregiving responsibilities or needs • Existing functional limitations • Recent role losses, bereavements • Individual risk factors • Sources of psychosocial support
AGE AND LIVING ARRANGEMENTS OF OLDER AMERICANS Source: Medicare Current Beneficiary Survey, 1997, Table 1.2.
SMALL IMPROVEMENTS CAN MAKE A BIG DIFFERENCE • For older patients, major changes in health or function may not be realistic • “Small” changes can transform quality of life: • regaining transfer ability can mean difference between returning home or to a nursing home • regaining ability to oppose thumb and fingers can mean difference between eating independently and being fed