Download
1 / 36
390 likes | 809 Views
Electrolytes. Hyponatremia. What is the serum osmolarity? 2(Na+) + BUN/2.8 + Glucose/18 Hyper-osmolar (>290) Hyperglycemia Mannitol Iso-osmolar (270-290) Hyperproteinemia Multiple myeloma Amyloidosis MGUS Hyperlipidemia

E N D
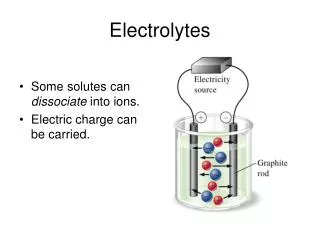
Hyponatremia • What is the serum osmolarity? • 2(Na+) + BUN/2.8 + Glucose/18 • Hyper-osmolar (>290) • Hyperglycemia • Mannitol • Iso-osmolar (270-290) • Hyperproteinemia • Multiple myeloma • Amyloidosis • MGUS • Hyperlipidemia • Hyper & Iso-osmolar hyponatremia is also called pseudo-hyponatremia
Hyponatremia • Hypo-osmolar • What is the volume status on physical exam • Hypovolemic • Dehydration • Vomiting • Diarrhea • Treat by calculating and replacing the sodium deficit • body wt in kg x 60% x 10meq • Select your IV fluid and rate • Watch for central pontine myelinosis during correction • Hypervolemic • CHF • ESLD • Nephrotic syndrome
Hyponatremia • Euvolemic • Addison’s disease • Drugs • HCTZ • SSRI • ACE-I • Hypothyroidism • Psychogenic polydipsia • SIADH
Hyponatremia • SIADH • Etiology • Pulmomary • Small cell carcinoma • TB • Pneumonia • Lung Abscess • CNS • Head injury • CVA • Meningitis / Encephalitis • Drug • Vincristine • Cyclophosphamide • Carbamazepine
Hyponatremia • SIADH • Diagnosis • Urine Sodium or osmolarity • Both should be elevated • Treatment • Treat the underlying cause • Fluid restriction • Demeclocycline • Vaprisol
Hypernatremia • What is the volume status • Hypovolemic • Dehydration • Vomiting • Diarrhea • Insensible and sweat losses • Treatment • Calculate the free water deficit • Total body water x (serum Na+ -140)/140 • Careful for cerebral edema during correction • Hypervolemic • Conn’s syndrome • Renin to Aldosterone ratio
Hypernatremia • Euvolemic • Diabetes Insipidus • Central DI • ADH insufficiency • Caused by • Neoplasm • Infiltrative lesions • Surgery • Radiotherapy • Head injury • Nephrogenic DI • ADH resistance • Caused by • Sickle cell disease • Pyelonephritis • Drugs: lithium, demeclocycline, colchicine
Hypernatremia • Diabetes Insipidus • Diagnosis • Compare plasma and urine osmolarity after dehydration (water deprivation test) and after vasopressin • Treatment • Central DI • Hormone replacement with vasopressin • Nephrogenic DI • HCTZ or amiloride enhances the reabsorption of fluid from the proximal tubule
Hyperkalemia • INCREASED POTASSIUM RELEASE FROM CELLS • Pseudohyperkalemia • Mechanical trauma during venipuncture • Cooling of the sample and specimen deterioration because of increased length of storage • May also represent severe intravascular hemolysis rather than a hemolyzed specimen • Marked leukocytosis or thrombocytosis (white cell or platelet count greater than 100,000 per mm3 or 400,000 mm3, respectively), as may occur with leukemia or a myeloproliferative disease
Hyperkalemia • INCREASED POTASSIUM RELEASE FROM CELLS • Metabolic acidosis • Insulin deficiency • Increased tissue catabolism • Any cause of increase tissue breakdown result in the release of potassium into the extracellular fluid • hyperkalemia may occur in this setting, particularly if renal failure is also present • Clinical examples include trauma
Hyperkalemia • INCREASED POTASSIUM RELEASE FROM CELLS • Beta-adrenergic blockade • Exercise • Hyperkalemic periodic paralysis • Digitialis • Succinylcholine
Hyperkalemia • REDUCED URINARY POTASSIUM EXCRETION • Hypoaldosteronism • Type 4 RTA • Potassium-sparing diuretics • Renal failure • Effective circulating volume depletion
Hyperkalemia • Treatment • Antagonism of membrane actions of potassium • Calicum • Drive extracellular potassium into the cells • Insulin and glucose • Sodium bicarbonate, primarily if metabolic acidosis • Beta-2 adrenergic agonists • Removal of potassium from the body • Loop or thiazide diuretics • Dialysis, preferably hemodialysis if severe • Cation exchange resin • Sodium polystyrene sulfonate (Kayexalate)
Hypokalemia • Major causes • Decreased potassium intake • Increased entry into cells • An elevation in extracellular pH • Increased availability of insulin • Elevated Beta-adrenergic activity • Stress or administration of beta-agonists • Hypokalemic periodic paralysis • Marked increase in blood cell production • Administration of vitamin B 12 or folic acid to treat a megaloblastic anemia • Granulocyte-macrophage colony-stimulating factor (GM-CSF) to treat neutropenia • Hypothermia • Chloroquine intoxication
Hypokalemia • Major causes • Increased gastrointestinal losses • Vomiting • Diarrhea • Laxative abuse • Increased urinary losses • Diuretics • Primary mineralocorticoid excess • Hypomagnesemia • Amphotericin B • Bartter's or Gitelman's syndrome • Increased sweat losses • Dialysis • Plasmapheresis
Hypokalemia • Treatment • 10 meq KCl will raise serum K+ by 0.1 • Be careful in renal failure
Hyperphosphatemia • Causes • MASSIVE ACUTE PHOSPHATE LOAD • Tumor lysis syndrome • Rhabdomyolysis • Lactic and ketoacidosis • Exogenous phosphate • Renal failure • Increased tubular reabsorption of phosphate • Hypoparathyroidism • Acromegaly • Due to insulin-like growth factor • Vitamin D toxicity • Bisphosphonates • Pseudohyperphosphatemia • hyperglobulinemia
Hypophosphatemia • Major causes • Internal redistribution • Increased insulin secretion • Refeeding syndrome • Hungry bone syndrome • Decreased intestinal absorption • Inadequate intake • Antacids containing aluminum or magnesium • Steatorrhea and chronic diarrhea • Vitamin D deficiency or resistance • Increased urinary excretion • Hyperparathyroidism • Vitamin D deficiency or resistance
Hypophosphatemia • Signs and symptoms • Mineral metabolism • Release of bone calcium contributes to the hypercalciuria • More prolonged hypophosphatemia leads to rickets and osteomalacia due to decreased bone mineralization • CNS • Metabolic encephalopathy • Confusion, seizures, delirium, and coma • CVS • Myocardial contractility may be impaired with ATP depletion • The reduction in cardiac output may become clinically significant, leading to congestive heart failure, when the plasma phosphate concentration falls to 1.0 mg/dL
Hypophosphatemia • Signs and symptoms • Skeletal and smooth muscle • Proximal myopathy, dysphagia and ileus • Hematologic dysfunction • Hypophosphatemia can also affect each of the components of the hematopoietic system • Treatment • Oral (Neutra-Phos) • IV (K-Phos)
Hypermagnesemia • Causes • Renal failure • Magnesium infusion • Severe preeclampsia or eclampsia • Oral ingestion • Magnesium enemas • Substantial quantities of magnesium can be absorbed from the large bowel • Among patients with renal failure, the administration of a magnesium enema can be fatal
Hypermagnesemia • Treatment • Most cases of symptomatic hypermagnesemia can be prevented by anticipation • Dialysis • When the toxic effects of magnesium must be reversed more quickly in a patient with severe symptoms, intravenous calcium can be given as a magnesium antagonist
Hypomagnesemia • Causes • GI losses • Renal losses • Both loop and thiazide diuretic can inhibit net magnesium reabsorption • Alcohol • Appears to reflect alcohol-induced tubular dysfunction that is reversible within four weeks of abstinence • Hypercalcemia • Calcium and magnesium seem to compete for transport in the thick ascending limb of the loop of Henle • Nephrotoxins • Aminoglycoside • Amphotericin B • Pentamidine • Cyclosporine • Loop of Henle or distal tubule dysfunction • Bartter’s syndrome
Hypomagnesemia • Signs and symptoms • Neuromuscular • Tetany • Positive Chvostek and Trousseau signs, and generalized convulsions • Can occur in the absence of hypocalcemia • Hypokalemia • Bone and calcium metabolism • PTH resistance • Vitamin D deficiency • CVS • Severe magnesium depletion can lead to prolongation of the PR interval, progressive widening of the QRS complex, and diminution of the T wave • Treatment • PO or IV replacement • Usually under treated
Serum Calcium • Normal value • 8.0 to 10.0 • Total body calcium • 99% in stored in bone • 1% in extracellular fluid • 3 forms of calcium in the blood • Bound to protein (40%-45%) • Correct for albumin • Free ionized (45-50%) • Order ionized calcium • Bound to anions (5-10%) • Phosphate, bicarbonate, citrate
Calcium physiology • Calcium is: • Absorbed from the gut • Stored in the bone • Excreted by the kidneys • Three endogenous chemicals regulate serum calcium • Parathyroid (PTH) • 1,25-(OH)2-D3 (Vit D) • Calcitonin • From the thyroid C cells • Can be considered a PTH antagonist • It slows down the osteoclasts causing a decrease in bone resorption
Calcium physiology • Decrease serum calcium, by reduced negative feedback, causes • Increased PTH • Causes a release of bone calcium stores • Decreased renal excretion of calcium • Increases activity of kidney hydroxylase causing increased 1,25-(OH)2-D3 • Increased Vitamin D • Increases Calcium absorption from the gut
Symptoms (>11.5-12) Urinary Polyuria Polydipsia Nephrocalcinosis Renal failure CNS Personality disturbance Mental obtundation or coma Neuromuscular weakness Easy fatigability GI Anorexia Weight loss Constipation Nausea / vomiting Abdominal pain Pancreatitis CV Hypertension Arrhythmias Short QT Hypercalcemia
Hypercalcemia • Severe hypercalcemia (>15) • Medical emergency • IV fluids • Lasix • Bisphosphonates • Calcitonin
Hypercalcemia • Causes • Primary hyperparathyroidism • One gland hyperplasia (most common) • Hyperplasia of all four glands • Parathyroid cancer is a rare cause • Can also be part of the MEN 1 & 2 • Maliganancy (PTH like hormone) • Lung (Squamous Cell) • Breast • Myeloma • Activation of osteoclasts • Others • Granulomatos diseases (Sarcoid) • Vit D activation by macrophages • Familial benign hypocalciuric hypercalcemia • Drugs (lithium, Vit D, HCTZ, milk-alkali syndrome) • Immobility
Hypocalcemia • Etiology • Decreased PTH secretion • Thyroid surgery and loss of parathyroid glands • Hypomagnesemia • Alcholics • Patients with bowel disease • Magnesium is required to secrete PTH • Vitamin D deficiency • Osteomalacia • Called rickets when in occurs in youth • Loss of calcium • Occurs with pancreatitis • Severe hyperphosphatemia • Calcium chelates with the phosphate • PTH resistance • Pseudohypoparathyroidism • Albright's hereditary osteodystrophy
Hypocalcemia • Clinical findings • Neuromuscular • Tetany • Chvostek sign (percussion of CN VII) • Trousseau sign • Laryngospasm • Cramping • Seizures • CV • QT prolongation • Refractory CHF • hypotension
Hypocalcemia • Diagnosis • Suggested when the serum calcium is low • Check albumin • Check ionized calcium • PTH may be low or high depending on the etiology • Check serum magnesium • Management • In the acute stages IV calcium can be given • Maintenance therapy includes oral calcium