Download
1 / 58
590 likes | 758 Views
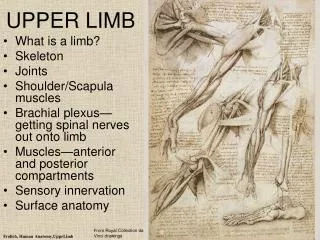
Upper Limb Musculoskeletal Surgery. Lisa Tourret MBChB.MSc.FRCS . FRCS (T&O) Nuffield Hospital Teaching Program. Aim. Introduction Scope of talk Selected conditions Shoulder Elbow Wrist Hand Questions and Answers. Who am I?. Lisa Tourret ( www.shoulder2hand.com )

E N D
Upper Limb Musculoskeletal Surgery Lisa Tourret MBChB.MSc.FRCS. FRCS (T&O) Nuffield Hospital Teaching Program
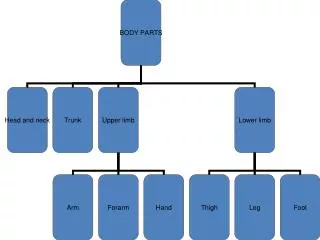
Aim • Introduction • Scope of talk • Selected conditions • Shoulder • Elbow • Wrist • Hand • Questions and Answers
Who am I? • Lisa Tourret ( www.shoulder2hand.com ) • Higher surgical training in Northern Region • Fellowships in New Zealand • North Shore Hospital • Middlemore Hospital • Consultant at SRH since 2006 • Relocated to Brighton August 2012
Scope of Talk • Common conditions of upper limb • Traumatic – accidental/sports injury • Degenerative – joint disease/ soft tissues • Neoplastic
Rotator cuff tear Calcific tendinopathy Impingement Cervical spine Shoulder Pain
Clinical Presentation - History • Shoulder pain - severity • Diffuse • Radiation? • Night pain • Aggravating factors • Relieving factors • Duration • Onset spontaneous or post trauma? • Age of patient
Clinical Presentation - Examination • Observe (symmetry, posture, muscle bulk…) • Palpation • Active movements (range, pain, scapulohumeral rhythm…) • Passive movements • Power against resistance • Impingement signs • Scarf and Obrien’s test • Stability
Jobe test and Hawkins sign Beware the patient with MDI presenting with impingement pain
Partial thickness tears • “Not a singular condition…rather a common outcome of a variety of insults to the rotator cuff.” AAOS vol 7 Jan 1999 • Aging (<40 yrs do not have tears, 25% of >60yr old do) • Anatomic impingement • Repetitive microtrauma
Partial thickness tears • Articular surface (2-3 times more common) • Bursal surface • Within tendon substance • Supraspinatus tendon most commonly involved • ?Progression ?Healing • 40 PTRCT at 1 year re-’scoped 11 progressed and 4 had healed Clin Orth 1994, 304
Full Thickness Rotator Cuff Tear • Small <1 cm • Moderate 1-3 cm • Large >3 cm • Massive > 5 cm • Surgery more successful in <4 cm
Calcific Tendonitis • Common disorder • Unknown aetiology • Multifocal cell mediated calcification • Spontaneous phagocytic resorption • Acute Pain during resorption phase • Not purely degenerative as it peaks in 5th decade and fully heals • Surgical removal is the exception not the rule (AAOS vol 5, no 4 1997)
Treatment Physiotherapy, NSAID, Injections, Arthroscopy, Debridement, Repair, Reconstruction, Replacement
Dislocation of Shoulder • First time traumatic • Recurrent • When is it recurrent? • What do we do? • Arthroscopic stabilisation – in whom? • Open stabilisation – in whom? • Bony reconstruction?
Frozen Shoulder • Adhesive capsulitis • Onset • Age • Duration • Natural time course (freezing/Frozen/Thawing) • When do we intervene? Distension or capsular release • IDDM?
Elbow • Tennis elbow • Ulna nerve compression or cubital tunnel syndrome • Loose bodies – locking • Stiffness – post traumatic? Arthritic? • Olecranon bursitis
Tennis elbow • Lateral epicondylitis • Radial tunnel syndrome • Resisted supination? • Middle finger test? • Injection site? • Surgical intervention <20% of initial presenters
Ulnar nerve compression • Cubital Tunnel Syndrome • 2nd only to Carpal Tunnel Syndrome • When to treat? • Non-operative measures • Operative – decompression vs transposition
Elbow Arthroscopy • Loose bodies • Arthrolysis • Tennis elbow • Osteochondritis • Synovectomy
Wrist and Hand • Carpal tunnel syndrome • Dupuytrens disease • Ganglions • Trigger finger • OA • Tendon sheath tumours – GCT, pea ganglions
When to treat? • Mature cords • MCP 30º • PIP 30º • Tabletop test
Ganglions • Symptomatic? • Lump or scar? • Recurrence rate • Complications
Trigger finger • Pathology? • Treatment • A1 pulley release • Recurrence? • Tendon slip excision
Hand tumours • More than 95% Benign • Occasional rare site for metastasis eg breast, lung • Primary malignant tumour very, very rare • Commonest are ganglia then Giant cell tumour of tendon sheath
Incidence of OA of the Hand • Commonest form of OA • <40 yrs - 50 new cases per 1000 person-years at risk • 40 - 59 yrs - 65 new cases per 1000 person-years at risk • >60 yrs - 110 new cases per 1000 person-years at risk (Kallman et al. 1990, Arth Rheum 33,1323 - 1332)
Surgical intervention • When non-operative methods fail • Fusion • Excision arthroplasty • Joint replacement • Interpositional arthroplasty
Distribution • DIPJ – fusion • 1st CMC –Trapeziectomy • PIPJ – fuse or replacement • MCPJ - replacement • Others - Sesamoid, Trapezial Scaphoid/trapezoid, Pisiform-triquetral OA