Download
1 / 20
200 likes | 488 Views
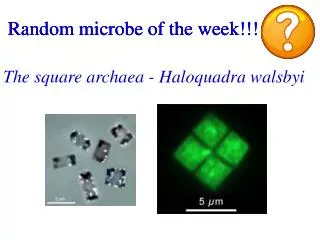
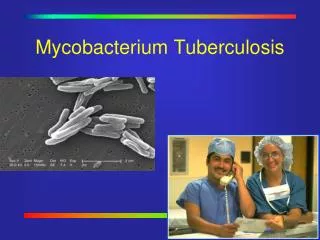
Microbe of the Week Mycobacterium marinum. The aquarium or fish tank disease,first reported in 1962 Rare but important if not treated Living example-Karen Bahr the Biology Department Administrative Assistant. Mycobacterium marinum Infection.

E N D
Microbe of the WeekMycobacterium marinum • The aquarium or fish tank disease,first reported in 1962 • Rare but important if not treated • Living example-Karen Bahr the Biology Department Administrative Assistant
Mycobacterium marinumInfection • Commonly found in aquariums and infected fish, reptiles or amphibians • Never transmitted from an infected human to another human
How do I get the Infection? • ・when in contact with water from an aquarium or fish tank • when handling, cleaning, or processing fish • while swimming or working in fresh or salt water.
Mycobacterium marinuminfection • Contracted when small cuts or abrasions exposed to aquarium water or fish amphibians etc • Usually results in superficial nodulars or ulcerated lesions on hands and fingers in the case of aquarium transmission • Swimming pool transmission same symptoms on elbows, knees and feet.
Mycobacterium marinum Infection
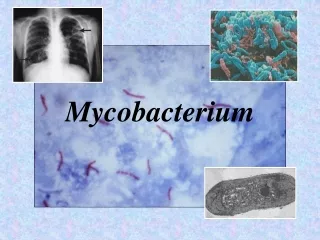
Mycobacterium marinumDiagnosis • Hardest part is the diagnosis. Difficult to culture using normal diagnostic media and incubation temperature and often goes undiagnosed for long periods • Culture on Mycobacterium medium called Lowenstein-Jensen or LJ at 32C. Will not grow at 37C • It is photochromogenic which means it produces a pigment when exposed to light thus this is diagnostic
Mycobacterium marinumDiagnosis • After culturing do an acid fast stain and then antibiotic susceptibility
Mycobacterium marinumTreatment • Surgical aspiration often done • Antibiotic treatment often for 2-12 months. • Minocycline combined with rifampin(rifamicin). Most potent rifamycins +clarithromycin • Wound dressing often silver based with collagen
Mycobacterium marinumPrognosis • Excellent recovery if treated with antibiotics and surgery • If untreated can lead to death
MICROBE OF THE WEEK Infection usually results because of antibiotic therapy which disturbs normal bacterial flora of colon. Cause- C. difficile releases 2 toxins, A and B. A is an enterotoxin and B is a cytotoxin. Both bind to receptors on the intestinal mucal cells compromising fluid absorption + retention
MICROBE OF THE WEEKClostridium difficile Disposition to: Hospitalization, antibiotic therapy, Age (elderly). Most common antibiotics implicated are chephalosorins, ampicillin/amoxicillin and clindamycin Mechanism: Spores of bacteria prevalent in hospitals. Ingestion or surgical contamination of patient. Spores germinate in colon and colonize producing toxins.
MICROBE OF THE WEEK Symptoms. Mild to moderate watery diarrhea(rarely bloody) cramping, anorexia, fever, dehydration, abdominal tenderness. Diagnosis. Conclusive diagnosis depends on detection of toxin in stool. Fibroblast tissue culture-24-48h(94-100%). Commercial enzyme immunoassay kits (69-87%). Less sensitive but very quick (hours)
MICROBE OF THE WEEK Treatment. Usually Vancomycin or Metronidazole. Organism is very susceptible to vancomycin. It is resistant to cephalosporins, ampicillin/amoxicillin, and clindamycin and aminoglycosides. Support therapy. Hydration.
MICROBE OF THE WEEK HELICOBACTER PYLORI AND PEPTIC ULCERS 95% of peptic ulcers and gastritis Also correlation between infection and gastric cancer
Helicobacter pylori Gram negative spirochete Colonizes gastric mucous secreting cells •Grown best under microaerophilic conditions •Causes disease via urease, proteases and phospholipase combined with a cell mediated immune response •50% of world population infected
Helicobacter pylori Gram negative spirochete Colonizes gastric mucous secreting cells •Grown best under microaerophilic conditions •Causes disease via urease, proteases and phospholipase combined with a cell mediated immune response •50% of world population infected
Helicobacter pylori Gram negative spirochete Colonizes gastric mucous secreting cells •Grown best under microaerophilic conditions •Causes disease via urease, proteases and phospholipase combined with a cell mediated immune response •50% of world population infected
Helicobacter pylori Identification • a biopsy with subsequent culture • breath test for urea • stool antigen assays •urease detection in biopsy
Helicobacter Pylori Treatment •PeptoBismol combined with metronidazole and tetracycline or amoxicillin