Download
1 / 40
480 likes | 1.08k Views
Liver and pancreas. SYLLABUS: RBP( Robbins Basic Pathology ) Chapter s : The Liver and the Biliary Tract The Pancreas. Liver and pancreas. 182a Chronic cholecystitis 228 Gall bladder carcinoma 249 Metastatic carcinoma of the liver (small cell carcinoma)

E N D
Liver and pancreas SYLLABUS: RBP(Robbins Basic Pathology) Chapters: TheLiver and theBiliaryTract ThePancreas
Liver and pancreas 182aChronic cholecystitis 228Gall bladder carcinoma 249Metastatic carcinoma of the liver (small cellcarcinoma) 230Metastatic carcinoma of the liver (mucinouscarcinoma) 254Chronic hepatitis 253Liver cirrhosis (H&A, Masson) 252Miliary tuberculosis (liver) 250Hepatocarcinoma 250aCholangiocarcinoma246Acute pancreatitis
flashback Liver and pancreas 3 Acute hepatic congestion 5Chronic passive congestion of the liver 17 Liver steatosis (H&E) 18 Liver steatosis (Sudan III) 43Balser necrosis (enzymatic fat necrosis) 186Insuloma
Acute hepatic congestion flashback
Chronic passive congestion of the liver flashback
Liver steatosis (H&E) flashback
Liver steatosis (Sudan III) flashback
Chronic hepatitis Chronic persistent hepatitis (CPH) pattern: - lymphocyte-predominant inflammation without: - loss of hepatocytes immediately surrounding the portal region ("piecemeal necrosis") - more than slight fibrosis Chronic active hepatitis (CAH) pattern: - portal lymphocyte-predominant inflammation - piecemeal necrosis - inflammation extending outward beyond limiting plate of portal triad to involve periportal hepatocytes- some hepatocytes are simply entrapped by inflammation while others drop out (liquefaction necrosis)- acidophil cells (apoptotic) possible- eventually: bridging fibrosis and/or cirrhosis
Liver cirrhosis • bridging fibrous septae in the form of delicate bands or broad scars linking portal tracts with one another and portal tracts with terminal hepatic veins • parenchymal nodules containing proliferating hepatocytes encircled by fibrosis, with diameters varying from very small (<3 mm, micronodules) to large (several centimeters, macronodules) • disruption of the architecture of the entire liver • Active cirrhosis:- piecemeal necrosis- extra-portal inflammation • Specific cause can sometimes be determined, (eg for viral infection, hemochromatosis, Wilson's disease, alpha-1-antitrypsin deficiency, and alcohol, if alcoholic hepatitis present)
Hepatocarcinoma - range of appearances from hepatocytes with little atypia forming sinusoidal, trabecular, or possibly tubular structures (well-differentiated)... - ... to highly atypical hepatocytes in sheets (poorly differentiated) - complete loss of bile ducts and Kupffer cells - little sclerosis
Cholangiocarcinoma - glands with cuboidal to columnar atypical and pleomorphic cells - typical perineural and periductal growth pattern - often desmoplastic stroma - may contain signet cells
Metastatic carcinoma of the liver microscopic features depend on the type of the primary tumor: eg: - small cell carinoma (lung) - mucinous carcinoma (GI)
Miliary tuberculosis (liver) numerous small TB granulomas
Chronic cholecystitis (some use this diagnosis whenever gallstones are identified, whether chronic inflammation is seen or not, others require chronic inflammation) - chronic inflammatory infiltration features - Rokitansky's-Aschoff sinuses (diverticula with increased smooth muscle, related to chronic increase in lumenal pressure) usually present and may have associated bile granulomas - possibly endarteritis obliterans - „follicular cholecystitis”: same lesion with germinal centers in wall of gallbladder
Gall bladder carcinoma - neoplastic glands lined by highly atypical cuboidal cells - desmoplastic stroma often forms concentric surrounding fibrosis
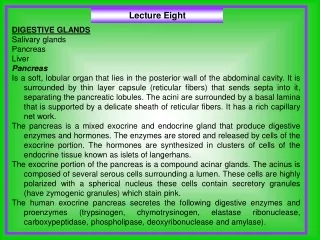
Acute pancreatitis Depending on the phase and severity: - acute inflammation - edema - fat necrosis - small vessel thrombosis - necrosis of acini - hemorrhages - extensive necrosis of both fat and parenchyma
Balser necrosis (enzymatic fat necrosis) flashback
Insuloma flashback