Download
1 / 1
10 likes | 253 Views
335-068. IMPROVING ACCESS TO CARDIOLOGY CONSULTATION. Ross A. Davies, Lorraine Clark, George A. Wells, Heather Sherrard, Lisa Jarvis, Terrence D. Ruddy and Robert S. Beanlands Divisions of Cardiology, Epidemiology and Nursing. Background

E N D
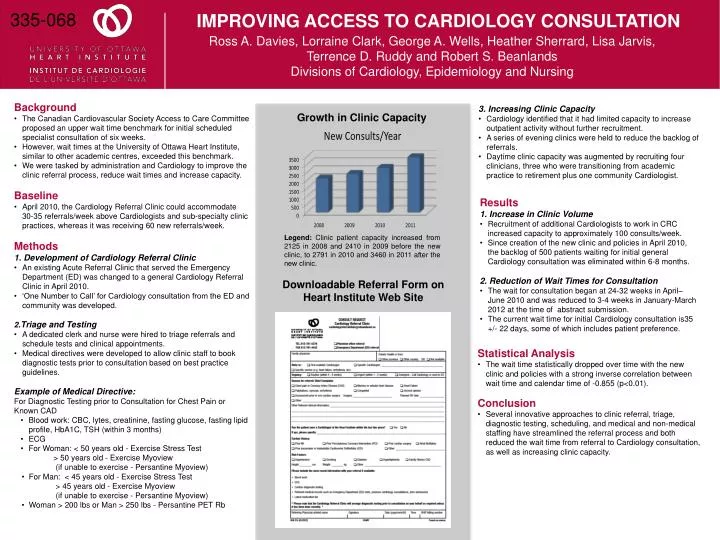
335-068 IMPROVING ACCESS TO CARDIOLOGY CONSULTATION Ross A. Davies, Lorraine Clark, George A. Wells, Heather Sherrard, Lisa Jarvis, Terrence D. Ruddy and Robert S. Beanlands Divisions of Cardiology, Epidemiology and Nursing • Background • The Canadian Cardiovascular Society Access to Care Committee proposed an upper wait time benchmark for initial scheduled specialist consultation of six weeks. • However, wait times at the University of Ottawa Heart Institute, similar to other academic centres, exceeded this benchmark. • We were tasked by administration and Cardiology to improve the clinic referral process, reduce wait times and increase capacity. • Baseline • April 2010, the Cardiology Referral Clinic could accommodate 30-35 referrals/week above Cardiologists and sub-specialty clinic practices, whereas it was receiving 60 new referrals/week. • Methods1. Development of Cardiology Referral Clinic • An existing Acute Referral Clinic that served the Emergency Department (ED) was changed to a general Cardiology Referral Clinic in April 2010. • ‘One Number to Call’ for Cardiology consultation from the ED and community was developed. • 2.Triage and Testing • A dedicated clerk and nurse were hired to triage referrals and schedule tests and clinical appointments. • Medical directives were developed to allow clinic staff to book diagnostic tests prior to consultation based on best practice guidelines. • Example of Medical Directive:For Diagnostic Testing prior to Consultation for Chest Pain or Known CAD • Blood work: CBC, lytes, creatinine, fasting glucose, fasting lipid profile, HbA1C, TSH (within 3 months) • ECG • For Woman: < 50 years old - Exercise Stress Test • > 50 years old - Exercise Myoview • (if unable to exercise - Persantine Myoview) • For Man: < 45 years old - Exercise Stress Test • > 45 years old - Exercise Myoview • (if unable to exercise - Persantine Myoview) • Woman > 200 lbs or Man > 250 lbs - Persantine PET Rb • 3. Increasing Clinic Capacity • Cardiology identified that it had limited capacity to increase outpatient activity without further recruitment. • A series of evening clinics were held to reduce the backlog of referrals. • Daytime clinic capacity was augmented by recruiting four clinicians, three who were transitioning from academic practice to retirement plus one community Cardiologist. Growth in Clinic Capacity • Results1. Increase in Clinic Volume • Recruitment of additional Cardiologists to work in CRC increased capacity to approximately 100 consults/week. • Since creation of the new clinic and policies in April 2010, the backlog of 500 patients waiting for initial general Cardiology consultation was eliminated within 6-8 months. • 2. Reduction of Wait Times for Consultation • The wait for consultation began at 24-32 weeks in April–June 2010 and was reduced to 3-4 weeks in January-March 2012 at the time of abstract submission. • The current wait time for initial Cardiology consultation is35 +/- 22 days, some of which includes patient preference. Legend: Clinic patient capacity increased from 2125 in 2008 and 2410 in 2009 before the new clinic, to 2791 in 2010 and 3460 in 2011 after the new clinic. Downloadable Referral Form on Heart Institute Web Site • Statistical Analysis • The wait time statistically dropped over time with the new clinic and policies with a strong inverse correlation between wait time and calendar time of -0.855 (p<0.01). • Conclusion • Several innovative approaches to clinic referral, triage, diagnostic testing, scheduling, and medical and non-medical staffing have streamlined the referral process and both reduced the wait time from referral to Cardiology consultation, as well as increasing clinic capacity.