Download
1 / 65
840 likes | 2.59k Views
PCOS new concepts and treatment. Peking University Third Hospital, P.R.China Qiao Jie. PCOS. The most common endocrine disorder Affecting about one in 15 reproductive age women worldwide Heterogeneous presentation Features : clinical and/or biochemical hyperandrogenism

E N D
PCOS new concepts and treatment Peking University Third Hospital, P.R.China Qiao Jie
PCOS • The most common endocrine disorder • Affecting about one in 15 reproductive age women worldwide • Heterogeneous presentation • Features: • clinical and/or biochemical hyperandrogenism • ovulatory dysfunction • polycystic ovaries
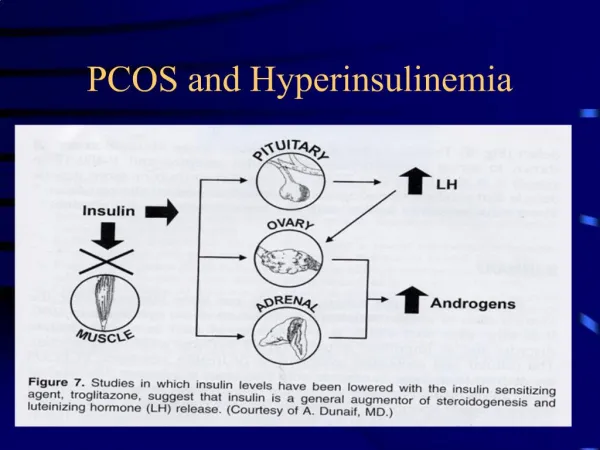
PCOS • Leading cause of androgen excess and ovulatory dysfunction • Causes 70–80% of hyperandrogenism • Obesity • LH/FSH> 2 or 3 • Insulin resistance (IR) • Impaired glucose tolerance (IGT) • Type 2 diabetes mellitus (DM) • Dyslipidemia and cardiovascular disease BRADLEY TRIVAX, MD CLINICAL BSTETRICS AND GYNECOLOGY Volume 50, Number 1, 168–177
PCOS symptoms and signs Robert J Norman, Lancet 2007; 370: 685–97
Criteria • The 1990 National Institutes of Health (NIH) criteria • Clinical hyperandrogenism and/or hyperandrogenemia • Oligo-ovulation or anovulation • Exclusion of related disorders Zawadzki J Boston: Blackwell; 1992. pp. 377–384
Criteria • 2003ESHRE/ASRM Rotterdam consensus meeting(Include 2 of the following) • Oligo- or anovulation • Clinical and/or biochemical signs of hyperandrogenism • Polycystic ovary morphology • Exclusion of related disorders The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Fertil Steril 2004; 81:19–25
Phenotypes • 2003 Rotterdamexpanded the definition of PCOS, adding two additional phenotypes 1) polycystic ovaries and clinical and/or biochemical evidence of androgen excess • without ovulatory dysfunction 2) polycystic ovaries and ovulatory dysfunction • without hyperandrogenemia and/or hirsutism (i.e. no signs of androgen excess)
Controversy Whether these two phenotypes actually represent PCOS ?? • subtle endocrine and metabolic abnormalities • Conditions also present with polycystic-appearing ovaries and ovulatory dysfunction • Hypothalamicamenorrhea • Hyperprolactinemia • Pubertal development Bradley Trivax, Cilinic Bstetrics Gynecol 50(1) 168–177
Controversy Whether these two phenotypes actually represent PCOS ?? • Carmina studied normal ovulation with PCO, hyperandrogenism women : • degrees of hyperinsulinism and hyperandrogenemia significantly less than NIH 1990 criteria PCOS • whether increased risk for developing metabolic complications, including type 2 DM, is not known Carmina E Hum Reprod. 2009 Sep;24(9):2286
Phenotype (based on 2003Rotterdam criteria) Robert J Norman, Lancet 2007; 370: 685–97
Phenotype (based on 2003Rotterdam criteria) Robert J Norman, Lancet 2007; 370: 685–97
Criteria • AES 2006 (include all of the following) • Hyperandrogenism(hirsutism and/or hyperandrogenemia) • Ovarian dysfunction(oligo-anovulation and/or polycystic ovary) • Exclusion of related disorders AES opinion: A principal conclusion was that PCOS should be first considered a disorder of androgen excess or hyperandrogenism Ricardo AzzizThe Journal of Clinical Endocrinology & Metabolism 91(11):4237–4245
Prevalence • Different in various race and ethnicity • US: Blacks 8.0 % and Whites 4.8% • Spain :6.5% • Greek :6.8% • Higher : Immigrant Indian subcontinent Aboriginal heritage Australian • according to the definition of PCOS used • the 2003 Rotterdam criteria is broader than 1990 NIH criteria: 1.5-fold higher Robert J Norman Lancet 2007; 370: 685–97
Hyperandrogenism • most important features of the syndrome • classic PCOS phenotype : higher androgen levels • clinical features ——hirsutism, acne, male-pattern alopecia • Biochemical ——testosterone ↑, DHEAS↑ androstenedioneor ↑, SHBG ↓
Hyperandrogenism • high circulating T concentrations: 60–80% • high DHEAS concentrations: 25% • Mornitoring indicators: • serum total testosterone • Bioavailabletestosterone (BioT) • SHBG • FAI • other androgens • assays inconsistent among individual laboratories Kumar A (PCOS). Clin Endocrinol 2005; 62: 644–49.
Hyperandrogenism • Do not allow monitor hormonal bioactivity • FAI (total testosterone/SHBGX100) • correlates with BioT • less overlap with normality • prostate-specific antigen —— promising marker of hyperandrogenism • strong positive correlation with testosterone and negative with SHBG levels
Clinical androgen excess • Hirsutism——70% • Acne——30% • Alopecia——8% • Hirsutism typically starts in the decade between 15 and 25 years and progresses slowly to become noticeable after 1 year from its onset • the prevalence of hirsutism in PCOS may vary according to race and ethnicity
Hirsutism • Ferriman-Gallwey (mFG) score (individual variation in hair growth may reflect ethnic differences) • positive FG≥6
The characteristics of hyperandrogenism in Chinese Han community population
Peking University Third Hospital • Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University • West China Second University Hospital, Sichuan University • First Affiliated Hospital of Medical College of Xi’an Jiaotong University • First Affiliated Hospital of Heilongjiang Chinese Medicine University • First Affiliated Hospital of Anhui Medical University • Tianjin Medical University General Hospital • Shengjing Hospital of China Medical University • Second Xiangya Hospital of Central-South University • Women’s Hospital of Fudan University • Women’s Hospital School of Medicine Zhejiang University • National center for chronic and noncomunicable disease control and prevention (NCNCD)
Introduction • Hyperandrogenism or androgen excess is a common endocrine disorder of adult women, affecting between 5 and 10% of women of reproductive-age • Hyperandrogenism comprises a heterogeneous group of disorders • Patients with hyperandrogenism present with a variety of clinical manifestations, include hirsutism, acne, androgenic alopecia, and virilization • Biochemical derangements in ovarian, adrenal, and peripheral androgen production • At present, there isn’t a widely accepted criteria for the diagnosis of hyperandrogenism of Chinese women
Objectives • The objective of our research is trying to provide the clinical and biochemical diagnostic criteria for the hyperandrogenism of Chinese women, hoping that it will provide an insight into the hyperandrogenism of yellow race women.
Methods and Materials • From Oct, 2007 to Sept. 2009 • A large-scale epidemiological investigation of reproductive-age women, aged 19 to 45 years old, in 10 provinces of China • Approved by ten centers and National center for chronic and noncomunicable disease control and prevention (NCNCD) • A total number of 10120 women from rural and urban communities, rural and urban 1:1 and 80-120 residents per community
We trained 20 interviewers (10 senior and 10 junior gyneocologists and postgraduate students) from university hospitals • All the fieldworkers completed training in their region, including pilot interviews in non-sampled communities • During fieldwork, the principal investigator and supervisors monitored interviews on site
All the participants underwent a free medical evaluation, including a self-history and family history, physical and pelvic examination, transvaginal ultrasonography • Part of the participants contributed their blood samples for determination of biochemical indicators • The women who were suffering from chronic or acute diseases, menopausal (including natural and surgical menopause), pregnant at the time were excluded from our study
Acne (Reingold and Rosenfield, 1987) • The scoring of acne is based on the evaluation of the papules, pustules and nodules of acne on the cheeks, neck, chest and upper back • The severity of acne was graded according to the Consensus Conference on Acne Classification • According to these criteria, mild acne is defined by the presence of comedones, without significant inflammation and a few or no papules; moderate acne, by the presence of comedones, with marked inflammatory papules and pustules; and severe acne, by the presence of inflammatory nodules, in addition to comedones, papules, and pustules
Blood samples • Sex hormone binding globulin (SHBG) • Total testosterone (TT) • Androstenedione (A) • Immulite 1000 assay based on chemiluminescence (DPC, USA) • Free androgen index (FAI) was calculated using the formula [TT (nmol/L) *100/SHBG (nmol/L)]
Result General characteristics of the population investigated • A total number of 10120 women between 19 and 45 years old were entered into our study, and 3303 blood samples were collected • 5 groups, 19-24 years old 1131 women (11.2%), 25-29 years old 1856 (18.3%), 30-34 years old 2165 (21.4%), 35-39 years old 2853 (28.6%) and 40-45 years old 2115 (20.9%) • 84.3% of them have regular menstruation cycle • 8631 women (85.3%) with normal cycles of 21-35 days, 1161 women (11.5%) with the duration of the cycle exceeds 35 days and 328 women (3.2%) with the cycles less than 21 days • 376 women (3.7%) suffered from infertility
Hirsutism • The F-G sore of the majority was 0(69.4%) and 95.5% of the participants had an F-G score under 5. Meanwhile, there were 96.4% of the participants under 6, 97.0% under 7 and 97.5% under 8. According this, we divided the participants into hirsutism and non-hirsutism by 5 F-G score
According 5 F-G sore, General characteristics of hirsutism and non-hirsutism group
Contribution of different areas to hirsutism(percentage) upper lip > lower abdomen > chest > thighs > upper arms > upper back > upper abdomen > chin > lower back
Acne The acne score of the women was mainly 0 (90.3%) , 1 (7.0%) making up 97.3% of the women under the score of 2 ACNE: 2.7%
Alopecia The incidence of alopecia was 1.3%, only 129 participants involved 118 mild, 8 middle and 3 serious alopecia.
Hormonal hyperandrogenism characteristics of the population investigated • total testerone level 1.54±0.83nmol/L • total androstenedione level 9.98±4.46 nmol/L • free androgen index (FAI) 3.45±0.06()
Conclusion Criteria of Clinical evaluation for hyperandrogenism in Chinese people • F-G score >=5 more significent position: upper lip, lower abdomen and chest Different age women used different hyperandrogenism evaluation system? • Acne score >= 2 • Fewer have alopecia
Materials and Methods • Study protocol • Questionnaires, including: • personal and family medical history • To define suspected PCOS cases • Oligomenorrhea: ≥35 days • Clinical hyperandrogenism: mF-G score≥6, or have acne, or have premature alopecia, or have acanthosis nigricans • Polycystic ovary: either 12 or more follicles measuring 2–9 mm in diameter in at least one of the ovaries
Clinical examination • To detect peripheral blood: INS, FPG, T, TSH, TG, Cho, HDL, and LDL • Transvaginal ultrasound • Defining PCOS:the Rotterdam criteria, the presence of two or more of the following • Oligomenorrhea • Clinical and/or biochemical hyperandrogenism • PCO
Healthy risk • Metabolic syndrome • central obesity:waist≥80cm • At least two of the following • TG elevated:≥1.7mmol/L • HDL decreased:<1.29mmol/L • BP increased:SBP≥130mmHg or DBP ≥85mmHg • FPG increased:FPG≥5.6mmol/L • IR: HOMA-IR=FPG*fasting INS/22.5 • Alberti KGMM et al. Metabolic syndrome-a new world-wide definition. A Consensus Statement fom the International Diabetes Federation. 2006. Diabetes UK. Diabetic Medicine, 23, 469-480.
Materials and Methods • At the same time, we choose hospital PCOS from the corresponding region hospital from 19-45 years old • A total of 959 diagnosed PCOS women were recruited (hospital PCOS)
Phenotype define O+H, Oligomenorrhea and hyperandrogenism O+P, Oligomenorrhea and PCO H+P, Hyperandrogenism and PCO O+H+P, Oligomenorrhea and hyperandrogenism and PCO Results
PCOS prevalence in China Biochemical Hyperandrogenism:T>2.81nmol/L Results Table 1: prevalence of PCOS in China (only with elevated T)
To compare the distribution of PCOS subgroups between community PCOS and hospital PCOS Results