Download
1 / 86
860 likes | 986 Views
It is 1950. Dr. L. Craven specializes in treatment of arthritis. Many of his patients receive aspirin and he notes that the incidence of myocardial infarction (heart attack) is lower than expected in these patients.

E N D
It is 1950. Dr. L. Craven specializes in treatment of arthritis. Many of his patients receive aspirin and he notes that the incidence of myocardial infarction (heart attack) is lower than expected in these patients.
Craven LL: Acetylsalicylic acid, possible preventive coronary thrombosis. Ann. West. Med. Surg. 4:95-99, 1950. Craven LL: Experiences with aspirin (acetylsalicylic acid) in the nonspecific prophylaxis of coronary thrombosis. Miss. Valley Med. J. 75:38-44, 1953.
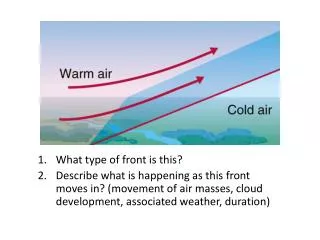
What type of study? • Case series • Case-control • Retrospective cohort • Prospective cohort • Clinical trial
Coronary Drug Project, 1976 • 1529 patients with a history of myocardial infarction, most of them several years earlier. • Randomly assigned (double-blind) to aspirin therapy - 324-mg tablet three times daily or placebo treatment. • Length of follow-up ranged from 10-28 months (average 22 months).
RR = 35/758 = 0.73 (0.48-1.11) 49/771 p=0.14 Interpretation? Conclusions? Coronary Drug Project, 1976 CHD Mortality Yes No 758 771 Aspirin Placebo How would you analyze these data? 4.6% 6.4%
Coronary Drug Project, 1976 Definite Non-fatal MI Yes No 758 771 Aspirin Placebo RR = 28/758 = 0.89 (0.54-1.45) 32/771 p=0.65 Interpretation? Conclusions?
Coronary Drug Project, 1976 “This difference is suggestive of a beneficial effect for aspirin in the treatment of post-MI men, but not large enough to be conclusive.”
Mayo Clinic Proceedings, 1978 Primary prevention in 473 patients with arthritis? • Followed arthritis patients on aspirin and determined MI, angina, stroke rates. • Compared to overall rates “in the community” (unpublished data). Overall, no difference in observed and expected rates of any outcome. However, in men there were 30-50% reductions (but NSD). MI in men: Expected 7.2; observed 5 (30% reduction)
A variety of case-control and cohort type studies with relatively small numbers of subjects suggested that aspirin might reduce coronary “events” by perhaps 20-30%, and it might be beneficial in primary prevention, but none of the observational studies had been conclusive. What were the major limitations of all of these observational studies? Small sample size; limited power to detect a modest difference Potential biases: misclassification, selection bias, recall bias Uncontrolled confounding: many other factors influence risk of heart disease
What should be done to determine whether aspirin is effective in primary prevention of cardiovascular disease? How would you do it?
Preventive RCTs Keep healthy people well Does tamoxifen lower the incidence of breast cancer in women with high risk profile compared to high risk women not given tamoxifen? Treat (or cure) disease Do combinations of 2 or 3 antiretroviral drugs prolong survival of AIDS patients better than single drugs? Therapeutic RCTs
New Drug Trials Phase I • Preliminary information on safety Phase II • Efficacy; dosage • Additional data on safety & side-effects Phase III • Advantage over existing treatments Phase IV • Post-marketing surveillance
Equipoise: Will the new treatment be better? Maybe; Maybe not. Sufficient doubt to justify withholding new treatment from some subjects. Sufficient belief to justify exposing some subjects to new treatment. Back to Aspirin – Is it ethical to do this?
Institutional Review Board Approval Required for all research involving human subjects (not just clinical trials). “Human Research” means a systematic investigation involving living humans (including research development, testing and evaluation), designed to develop or contribute to generalizable knowledge. Benefits Risks
Who should we invite to participate? (age, gender, occupation?) Inclusion/exclusion criteria?
Selection of Study Population Reference population–The general group to whom results should be applicable. • All humans • Women with breast cancer • Men at risk for MI • Study or experimental population– • Potential participants (people considered for enrollment). • Breast Cancer patients at BUMC • U.S. Physicians • U.S. Health Professionals
Are you going to use a placebo? Why or why not? Is it ethical to use a placebo?
Why Use A Placebo? • Minimize bias in assessing outcomes • Makes groups as comparable regarding the perception of treatment. • Allows “blinding” (not always possible).
Blinding (or Masking) Exposure status is unknown. • Minimizes bias in assessing outcomes • Single-blind: subjects unaware of treatment group • Double-blind: subjects and investigators unaware
211/317 = .666 = 67/100 From Clegg DO, et al.:Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med 354:795, 2006.
Glucosamine + Chondroitin: 211/317 = 67% Placebo: 188/313 = 60% The “placebo effect” What can you conclude? How would you go about making a formal comparison? From Clegg DO, et al.:Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med 354:795, 2006.
Statistical power: the ability of a study to demonstrate a statistically significant association, if one exists. • How many will have expected end points? Restrict study to persons at higher risk? • Duration of Follow-up: Is there sufficient time to accumulate end points? • Acute vs. long-term effects of treatment. • Do you need multiple study sites? Sample Size Estimates
What do we do after we have a group of willing subjects? Informed consent? (What is informed consent)?
Informed Consent • Informed about: • Treatments • Potential outcomes; risks/benefits • Randomization (i.e., treatment is not their choice) • What is required of them Obtain informed consent prior to randomization.
Randomization Method of assignment such that each individual has an equal chance of receiving each possible treatment. Equal chance: • Coin toss • Random numbers (table or computer) • Other methods have potential problems • Subject self-selects • Day of week, order of visit, etc. • Benefits/Strengths: • Unpredictability • Leads to comparability • Balance of known & unknown confounders • Minimizes selection bias
Large, carefully done randomized clinical trials are particularly useful for assessing moderate or small effects which may be clinically important. • Random assignment of a sufficiently large number of subjects provides exquisite control over both known and unsuspected confounding factors. • A large sample size increases the ability to identify modest, but significant differences.
Population Hierarchy Reference Population Experimental Population(potential participants) Non-participants Participants(willing and eligible) Allocation Active Intervention Group Comparison Group • Compliers • Non-compliers • Compliers • Non-compliers
Ok, so now the trial is under way and they plan to follow subjects for 8 years. Anything else we should do while we are waiting for the results?
What about maintaining compliance (adherence to the protocol) and follow up? Does compliance matter? What steps can you take to maintain compliance and follow up? How do you know if they have complied?
Maintaining Compliance & Follow-up • Following assigned protocol for the duration of the study is crucial to ability to demonstrate a true effect. • Noncompliance makes the groups more alike & reduces the ability to detect a difference (bias towards null). • Begin with a motivated, knowledgeable group. • Identify subjects who are unlikely / unable to comply. • Make the protocol as simple as possible. • Be clear about what is involved. • If possible, mask the treatment so all groups comply. • Maintain frequent contact with subjects without interfering with treatment. • Provide incentives (free check-ups, transportation, etc.) • Conduct a “run-in” or “lead-in” period before the real trial.
Assessing Compliance Assess compliance, if possible. • Self-report • Pill counts • Biological measures (blood, urine)
Non-compliance Tends to Bias Toward the “Null” “Null” means no difference 0.3 0.5 1.0 2 3 Relative Risk
Data and Safety Monitoring Board A scientifically & financially independent group with expertise in various disciplines charged with safeguarding participants. Reviews progress of trial & data on outcome • Interim results • Adverse events Can recommend modification or termination of all/part of trial. • Treatment results so good cannot withhold from others. • Treatment side effects/outcome so bad cannot continue.
Physicians' Health Study • Randomized, double-blind, placebo controlled trial. • Primary prevention of CVD & cancer in 22,071 U.S. male physicians, aged 40-84 at baseline. • A 2x2 factorial design to test: • 325 mg aspirin on alternate days • 50 mg beta carotene on alternate days
Physicians' Health StudyExclusion Criteria • History of: • Heart attack • Stroke • Cancer • Current liver or kidney disease • Peptic ulcer or gout • Contraindication to aspirin • Current use of aspirin or other drugs affecting platelet function • Current use of a vitamin A or b carotene
Physicians' Health Study 261,248 invitation letters sent with questionnaire 112,528 questionnaires returned 59,285 willing to participate 33,223 eligible and enrolled in 18-week run-in phase on active ASA & b-carotene placebo. 22,071 randomized
Aspirin11,037 Aspirin Placebo11,034 b-carotene5,517 b-caroteneplacebo5,520 b-carotene5,519 b-caroteneplacebo5,515 Randomization Scheme 2x2 factorial design 22,071 U.S. Male Physiciansaged 40-84 Both Aspirin b-carotene Neither
How can we tell if randomization was successful? What are some known risk factors for heart disease? Were these confounding factors distributed equally?
Baseline Characteristics Aspirin Placebo (n=11,037) (n=11,034) Age (yrs) 53.2 9.5 53.2 9.5Systolic BP (mmHg) 126.1 11.3 126.1 11.1Diastolic BP (mmHg) 78.8 7.4 78.8 7.4History of hypertension (%) 13.5 13.6History of high cholesterol (%) 17.5 17.3Cholesterol level (mg) 212.1 44.2 212.0 45.1History of diabetes (%) 2.3 2.2History of angina (%) 1.3 1.2Parental MI (%) 13.0 13.1
Baseline Characteristics Aspirin Placebo (n=11,037) (n=11,034) Current smoking (%) 11.0 11.1Past smoking (%) 39.4 39.1Daily alcohol (%) 24.9 25.0Exercise >1/week (%) 71.7 71.2Body mass index (kg/m2) 24.9 3.1 24.9 3.0Multivitamin 19.9 19.9
How will we analyze the data? Basic analysis is that of a cohort study (i.e. – compare incidence….) Should we include all subjects in the analysis?
Compliance After 60.2 months Placebo Group 14.23% took aspirin or other platelet-active drugs Aspirin group 85.71% took treatment as intended Who should we include in our analysis?
Intention to Treat Analysis Primary analysis: “Intention to treat” • For the primary analysis all subjects should be included in the groups to which they were randomly assigned, even if they did not complete or even receive the appropriate treatment. • Preserves baseline comparability & control of confounding • Since compliers and non-compliers may be systematically different it prevents bias. • It reflects efficacy in everyday practice. Secondary analysis: Compliers only. • Not a randomized comparison.
Fatal Myocardial Infarction Yes No 11,037 11,034 Aspirin Placebo Use “Epi_Tools.xls” to calculate the risk ratio, the p-value, & 95% CI. Interpret your findings in words.