Download
1 / 114
1.24k likes | 1.74k Views
Rectal Disorders. Victor Politi, M.D., FACP Medical Director, SVCMC School of Allied Health Physician Assistant Program. Anatomy. The rectum is the lower 10 to 15 cm of the large intestine.

E N D
Rectal Disorders Victor Politi, M.D., FACP Medical Director, SVCMC School of Allied Health Physician Assistant Program
Anatomy • The rectum is the lower 10 to 15 cm of the large intestine. • The anatomic anal canal is the outlet of the digestive system. It is a tube about 3.8 cm long running from the perianal skin of the buttocks to the mucosal lining of the rectum.
Anatomy • Its external opening is the anus, which is tightly shut except during stool evacuation by two strong but sensitive rings of muscles: the internal sphincter and external sphincter.
Anatomy • The action of the internal sphincter is controlled subconsciously (it is always contracted to prevent accidental loss of stool), whereas the action of the external sphincter is voluntary.
Anatomy • The sphincters are well supplied with blood vessels and nerves. • Where the anal canal meets the rectum there is a ring of folds called the dentate line. • Among these folds are the anal crypts, small tube-like depressions opening into the anal canal.
Anatomy • The dentate line delineates where nerve fibers end. • Above this line, this area is relatively insensitive to pain. • Below the dentate line, the anal canal and anus are extremely sensitive.
Anatomy • The veins from the rectum and anus drain into the portal vein, which leads to the liver, and then into the general circulation. • The lymph vessels of the rectum drain into lymph nodes in the lower abdomen; those of the anus drain into the lymph nodes in the groin.
Rectal Exam • Inspect the skin around the anus for any abnormality. • With a gloved finger, probe the rectum. • For women, this is often done along with a manual examination of the vagina.
Rectal Exam • An anoscope or proctoscope (a 3- to 10-inch rigid viewing tube) can also be used. • A sigmoidoscope (a longer, flexible tube) can observe as much as 2 or more feet of the large intestine. • An anoscopy or sigmoidoscopy is generally uncomfortable but not painful; however, if the area in or around the anus proves to be painful because of an abnormal condition, a local, regional, or even general anesthetic may be given before examination proceeds.
Rectal Exam • Sometimes a cleansing enema to rid the lower part of the large intestine of stool is given before sigmoidoscopy. • Tissue and stool samples for microscopic examination and cultures may be obtained during sigmoidoscopy. • A barium enema x-ray may also be performed.
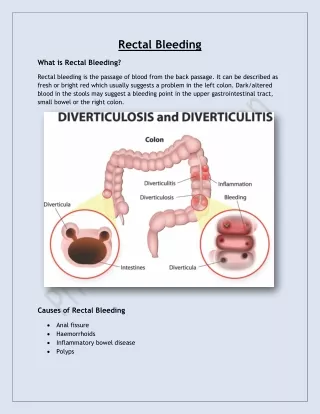
Hemorrhoids • Hemorrhoids are dilated, twisted (varicose) veins located in the wall of the rectum and anus.
Hemorrhoids occur when the veins in the rectum or anus become enlarged; they may eventually bleed. • Hemorrhoids may also become inflamed or may develop a blood clot (thrombus).
Hemorrhoids that form above the boundary between the rectum and anus (anorectal junction) are called internal hemorrhoids. • Those that form below the anorectal junction are called external hemorrhoids. • Both internal and external hemorrhoids may remain in the anus or protrude outside the anus.
Hemorrhoids • Cushions of vascular tissue found within the anal canal - when examined microscopically, lack a muscular wall • The lack of muscular wall characterizes these vascular structures more as sinusoids and not veins
Hemorrhoidal bleeding is actually arterial - although many still call it venous bleeding • Hemorrhage from disrupted hemorrhoids occurs from presinusoidal arterioles • Hemorrhoidal tissue is thought to contribute to anal continence and functions as a compressible lining that provides complete closure of the anus
The main cushions are primarily found anatomically in the left lateral, right anterolateral, and right posterolateral positions, with smaller accessory cushions in other quadrants
Etiology • Most common cause - constipation • Prolonged straining • Pregnancy • Heredity • Increased intra-abdominal pressure • Aging (due to thinning of supportive tissue)
The Liver and Hemorrhoids • Look at the venous return for the external and internal hemorrhoidal veins • External - systemic • Internal - portal
Classification • Internal Hemorrhoid • Whenever the internal hemorrhoidal plexus is enlarged, there is associated increase in supporting tissue mass with resultant venous swelling • External Hemorrhoid • The veins in the external hemorrhoidal plexus become enlarged or thrombosed, the resultant bluish mass is called an external hemorrhoid
Classification • Both types of hemorrhoids are very common and are associated with increased hydrostatic pressure in the portal venous system such as during pregnancy, straining at stool, or with cirrhosis
Classification • Internal vs. external • External are distal to the dentate line • Internal are proximal to the dentate line • Internal hemorrhoids are further sub-classified by their physical characteristics
Classification of Internal Hemorrhoids • Grade I • Seen on anoscopy, may bulge a short way into anal canal; does not extend below dentate line • Grade II • Prolapses out of anal canal with straining or defecation; reduces spontaneously • Grade III • Prolapses out of anal canal with straining or defecation; reduces manually • Grade IV • Irreducible;may strangulate
Generalized Symptoms • Bleeding on stool or in toilet • Mucosal protrusion • Discharge • Soiled underwear - due to internal • Sensation of incomplete evacuation
Generalized Symptoms • Hemorrhoids are painless unless thrombosed • Bleeding from internal hemorrhoids is bright red - from external - darker
Symptoms - Internal Hemorrhoids • When internal hemorrhoids enlarge pain is not a usual feature until complicated by thrombosis, infection, or erosion of the overlying mucosal surface • Most persons complain of bright red blood on the toilet tissue, or coating the stool, with a feeling of vague anal discomfort
Symptoms - Internal Hemorrhoids • The discomfort is increased when the hemorrhoid enlarges or prolapses through the anus • Prolapse is often accompanied by edema and sphincteric spasm • Prolapse, if not treated, usually becomes chronic as the muscularis stays stretched - the patient c/o constant soiling of underwear and very little pain
Symptoms - Internal Hemorrhoids • Prolapsed hemorrhoids may become infected or thrombosed; the overlying mucous membrane may bleed profusely as the result of trauma of defecation
Symptoms - external hemorrhoids • External hemorrhoids, because they lie under the skin are usually very painful • Result in tender blue swelling at the anal verge due to thrombosis of a vein in the external plexus - need not be associated with enlargement of the internal veins • Spasm often occurs since the thrombus usually lies at the level of the sphincteric muscles
Diagnosis • The diagnosis of internal or external hemorrhoids is made by • inspection • digital exam • direct vision through the anoscope & proctosocpe
Diagnosis • Exam- • Prone, jack-knife position or lateral Sim’s position • Location of the hemorrhoids should be described according to their anatomic position • Visual inspection • DRE- digital rectal exam
Diagnosis • Since hemorrhoids are very common, they must not be regarded as the cause of rectal bleeding or chronic hypochromic anemia until a through investigation has been made of the more proximal GI tract • Acute blood loss can occasionally be attributed to internal hemorrhoids • Chronic anemia in the presence of a large but not bleeding hemorrhoid should provoke a search for a poly, cancer or ulcer
Treatment • Treatment includes medical as well as surgical modalities • With medical therapy, bleeding and pain usually improve over a 6 week period
Treatment • Most hemorrhoids respond to conservative therapy such as sitz baths or other forms of moist heat, suppositories, stool softeners, and bed rest
Medical Therapy • Stool bulking agent • Psyllium • Methylcellulose • Sitz baths • probably most effective topical treatment for relief of symptoms
Treatment • Internal hemorrhoids that remain permanently prolapsed are best treated surgically; milder degrees of prolapse or enlargement with pruritus ani or intermittent bleeding can be successfully handled by banding or injection of sclerosing solutions
Treatment • External hemorrhoids which become acutely thrombosed are treated by incision, extraction of the clot, and compression of the incised area following clot removal • No surgical procedure should be carried out in the presence of acute inflammation of the anus, ulcerative proctitis, or ulcerative colitis
Treatment • Both proctoscopy and barium enema should always be performed before a patient is subjected to hemorrhoidectomy
Surgical Therapy • Rubber Band Ligation • One of most widely used techniques • Approximately 5-7 days after procedure the banded tissue sloughs-off • Infrared Photocoagulation • Laser not often used • Sclerotherapy • Phenol 5% • Sodium tetradecyl sulfate
Surgical Therapy • Operative hemorrhoidectomy • Indicated for patients with symptomatic combined internal and external hemorrhoids
Anal Inflammation • Perianal inflammatory lesions may be primary or may be associated with inflammatory bowel disease or diverticular disease • Anal fissures are superficial erosions of the anal canal which usually heal rapidly with conservative therapy
Anal Inflammation • Anal ulcers are more chronic and deep and give symptoms largely as the result of painful spasm of the external anal sphincter during and after defecation • Bleeding may occur with either fissure or ulcer • Healing of the ulcer is often associated with a hypertrophied anal papilla and some degrees of anal contracture
Anal Inflammation • Fistula in ano, a tract leading from the rectal lumen to the perianal skin, usually results from local crypt abscesses • fewer than 5% of these lesions found in the US are due to TB or cancer • The fistula is a chronically inflamed canal made up of fibrous tissue surrounding granulation tissue